

Background: Hydroxyurea (HU) therapy in sickle cell anemia (SCA) improves health care utilization, slows organ failure, and prolongs life. Implementation of evidence-based, comprehensive care has been shown to improve health-related quality of life (HRQOL). Case management by community health workers (CHWs) is an evidence-based health management strategy. We therefore hypothesized that HU-eligible SCA adults exposed to patient navigators (PN), CHWs specially trained as case managers for SCA, would have improved HRQOL compared with controls.
Methods: We enrolled 224 patients eligible for HU into the Start Healing in Patients with Hydroxyurea (SHIP-HU) Randomized Controlled Trial. All patients received care from trained physicians who implemented use of a standardized HU prescribing protocol using NIH guidelines. Pateints were randomized to either PN intervention (which included case management and education through home, telephone, and/or other visits from PNs) plus standard care by their treating physician (Experimental, E), or standard care by their physician alone (Control, C). Study physicians were blinded to study arm. At baseline, 6 and 12 months we assessed 4 psychosocial HRQOL variables-- ASCQ-Me emotional impact (EMOT), social impact (SOCI), PROMIS global mental (GMENT) and satisfaction with social roles (ROLE); 6 Physical HRQOL variables-- ASCQ-Me Sleep impact (SLEP) and Stiffness (STIFF), PROMIS global physical (GPHYS), Physical health (PHYS), Fatigue (FATG), and sleep/Wake disturbance (WAKE), and 4 pain HRQOL variables-- PROMIS pain behavior (PAINB), and ASCQ-ME-Pain crisis frequency (PAINF), Pain crisis severity (PAINS), and Pain impact (PAIN). Main analyses consisted of mixed model analysis of variance of follow-up visits, controlling for site and baseline value of outcome variable. Any missing baseline values for subjects were imputed.
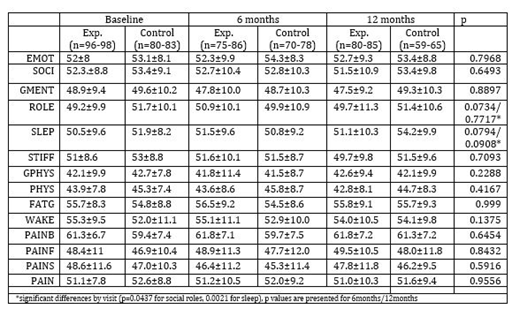
Results: 181 of 224 randomized patients had at least one HRQOL measure at follow-up. Patients had mean age 30.3, 45.3% were male, 81.2% were on HU at baseline. No HRQOL measures were different between groups E and C in any domain (Table, variables grouped by domain).
Conclusions: In our sample, there were no differences in HRQOL among patients who were exposed to PNs vs those who weren't. These findings require further analyes before firm conclusions can be made about the isolated effect of PNs on HRQOL. PN dose of intervention was likely variable. HU use and adherence has been associated with higher HRQOL, and we did not predict high baseline HU uptake and adherence which may have led to minimal improvement despite adequate PN intervention. PNs were not allowed to work with MDs, nor did they work with the remainder of the health care team to improve HRQOL. Analyses are underway to examine these and other possible influences on HRQOL.
Smith:Novartis: Consultancy, Honoraria. Villella:Emmaus: Membership on an entity's Board of Directors or advisory committees; Pfizer: Other: Site PI for the Rivipansel Clinical Trial. Liles:Novartis: Other: PI on clinical trial Sickle cell ; Shire: Other: PI on clinical trial Sickle cell ; Imara: Other: PI on Clinical trial- Sickle cell .

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal