


INTRODUCTION: Thrombophilia testing (TT) is ordered in acute ischemic stroke (AIS) in an attempt to diagnose rare hypercoagulable disorders, most notably antiphospholipid antibody syndrome (APS), as secondary stroke prevention may require anticoagulation in addition to antiplatelet therapy. Given the paucity of clinical evidence and the absence of formal guidelines, TT is frequently overused, resulting in excess health care costs and potential misinterpretation of results which may result in patient harm. Herein, we report the ordering practices and the effects of TT on outcomes in patients hospitalized for AIS at a large academic center, with the intent of identifying areas for intervention to improve TT stewardship.
METHODS: Patients hospitalized for AIS between January, 2015, and January, 2017, were identified using ICD-10 codes, and those that received TT were identified using laboratory records. Demographic, medical history, stroke diagnostic workup, and TT characteristics were collected from medical records. Distribution of variables were reported using mean (SD) or median (IQR) for continuous variables and percentages for categorical variables.
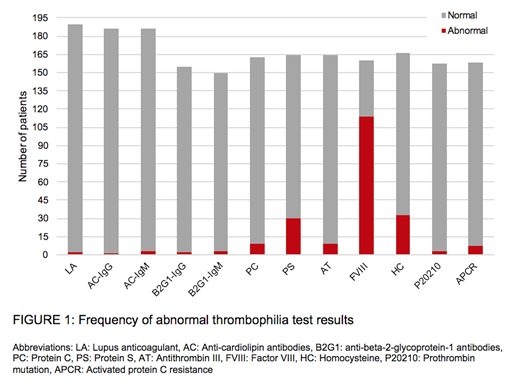
RESULTS: Of the 1900 patients admitted with AIS during this 2-year period, 190 (10%) underwent TT which included: lupus anticoagulant (100%), anticardiolipin IgG and IgM (97.9%), anti-beta-2-glycoprotein-1 IgG (81.6%) and IgM (78.9%), protein C (85.8%), protein S (86.3%), antithrombin (86.3%), factor VIII (84.2%), homocysteine (87.4%), prothrombin gene mutation (82.6%), and activated protein C resistance (83.2%). Of these, 137 (72.1%) had at least 1 abnormal result. However, when abnormal factor VIII (71.3% abnormal) was excluded, the percent with an abnormal result was 37%. Patients who underwent TT were younger compared to those who did not (mean age 47.3y, SD 13.8 vs. 64y, SD 15; p<.0001). Females were more frequently tested than males (60% vs. 40%). Testing of White and African American patients reflected the demographics of the stroke population (55.7% and 42.8%, respectively). Most tested patients (82%) had at least 1 cardiovascular disease risk factor based on the Framingham Heart Study risk algorithms.
Elevated factor VIII constituted the most common abnormal test, followed by elevated homocysteine (19.9%) and low protein S (18.3%) (Fig 1), though this testing is not recommended during acute thrombosis. At least one assay for APS was positive in 3 patients (1.6%), which was repeated in only 1 patient after 12 weeks. Testing for APS was incomplete in 23% of patients, most frequently due to the omission of anti-beta-2-glycoprotein-1 antibodies. Only 16% of patients received inpatient or outpatient hematology input, all after the TT had been ordered. The average time between admission and TT was 1.79 days, with 68.4% of patients tested within 24 hours of admission, indicating that TT was reflexive and occurred prior to evaluation for cardiovascular risk factors. The indication that prompted TT was not documented in 75.3%; most commonly documented indications were younger age (8%), personal (5%) or family history of thrombosis (7.7%), and a history of a rheumatologic disorder (4%). Documentation of family history was incomplete or absent in 31% of tested patients.
At discharge, the etiology of stroke was determined in 53.2% of the patients who underwent TT testing, while 46.8% remained undetermined. TT changed management in 4 patients (2%); 3 with APS and 1 with heterozygous factor V Leiden were started on anticoagulation. One patient subsequently developed a clinically relevant non-major bleeding and anticoagulation was discontinued.
CONCLUSION: We found that TT is frequently obtained in hospitalized patients with AIS, often before evaluation for other traditional stroke risk factors has been performed. TT changed management in only 2% of tested patients and contributed to harm in 1 patient. Collaboration between hematologists and neurologists to improve TT stewardship is needed to curtail patient risk and unnecessary cost. In an effort to limit TT, we are increasing awareness through provider education, and have created an order set in the electronic medical record to encourage appropriate ordering practices and consultation with hematology in patients with AIS where TT is felt to be indicated.
No relevant conflicts of interest to declare.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal