

BACKGROUND. In patients with cancer-associated venous thromboembolism (CAVT), recent randomized trials reported similar or improved efficacy of direct oral anticoagulants (DOACs) compared to standard-of-care low molecular weight heparin (LMWH) but noted increased bleeding in patients with gastrointestinal (GI) or genitourinary (GU) lesions. Both the National Comprehensive Cancer Network and the International Society on Thrombosis and Hemostasis have adapted guidelines on judicious use of DOACs in CAVT patients with GI or GU lesions. Differences in DOACs utilization may have significant impact on bleeding, recurrent thrombosis, and cost utilization. We sought to examine provider utilization and perception of different anticoagulants in CAVT.
METHODS. We examined DOAC utilization in CAVT patients and surveyed hematology/oncology providers within the Yale New Haven Health System that includes 5 hospitals, an NCI-designated cancer hospital with a network of 14 regional cancer care centers. The utilization of DOACs was examined retrospectively from January 2014 through December 2018 with data query tools built into the Epic electronic medical record used throughout the Health System. The 17-question online survey was administered in June-July 2018 to 90 providers and a year later, to 101 providers. The Qualtrics survey platform was used to record anonymous responses. No incentive was provided for responses. For statistical comparisons, we used chi-square tests of proportions.
RESULTS
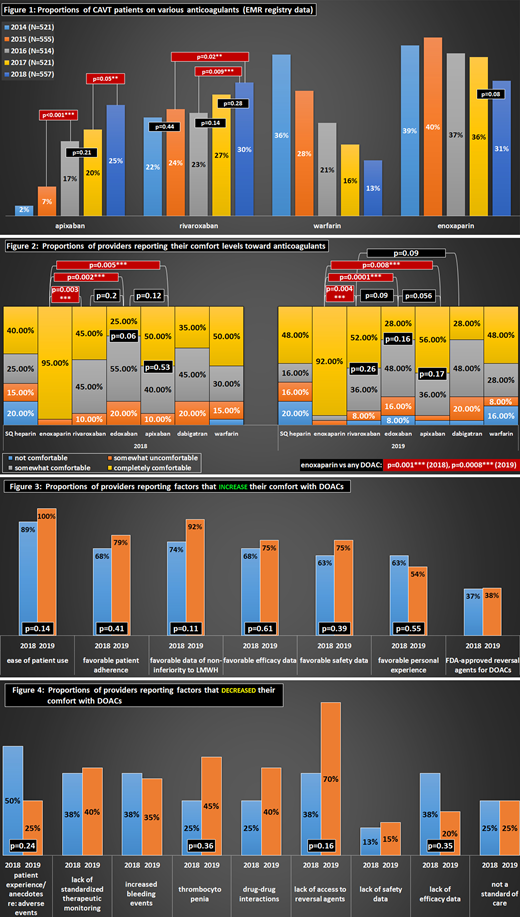
EMR: Use of rivaroxaban and apixaban rose from 22% to 30% and from 2% to 25%, respectively, while warfarin use dropped from 36% to 13%. Use of apixaban increased at a faster rate than that of rivaroxaban as indicated by statistically significant year-to-year changes for the former. Enoxaparin remained the most commonly used anticoagulant in CAVT, and although its use trended down, it remained similar throughout the study period (Fig 1).
SURVEY: The response rates for the two surveys were 22% in 2018 (22 respondents) and 25% in 2019 (25 respondents). Far more providers felt completely comfortable with enoxaparin than apixaban (2018: 95% vs 50%, p=0.005; 2019: 92% vs 56%, p=0.008) or rivaroxaban (2018: 95% vs 45%, p=0.003; 2019: 92% vs 52%, p=0.004). Among DOACs, more providers felt completely comfortable with apixaban (50% in 2018, 56% in 2019) and rivaroxaban (45% in 2018, 52% in 2019) than with edoxaban (25% in 2018, 28% in 2019) or dabigatran (35% in 2018, 28% in 2019) (Fig 2). Provider comfort level with different anticoagulants in CAVT did not change between the two survey periods.
Factors that added to the provider comfort level with DOACs included ease of patient use, favorable patient adherence and personal experience, favorable efficacy and safety data (Fig 3). Only a minority of providers (37% in 2018 and 38% in 2019) felt that the FDA approval of andexanet had an impact on their comfort level with DOACs in CAVT. At the same time, a majority of responders in 2019 (70%) identified lack of access to reversal agents as a factor that made them less comfortable (Fig 4). The majority of providers identified GI or GU lesions or instrumentation, active or major bleeding, brain lesions, and liver impairment as relative contraindications to DOAC use in CAVT. Only about half of providers felt that renal impairment (53% in 2018, 50% in 2019) or thrombocytopenia (53% in 2018, 42% in 2019) should be contraindications. The majority of providers (80% in 2018, 68% in 2019) felt that results of clinical trials of DOACs in CAVT made them more likely to use DOACs in CAVT.
CONCLUSIONS: The use of DOACs in treatment of CAVT is increasing and in our Health System accounts almost entirely for a decrease in warfarin use in CAVT, while the use of enoxaparin has not substantially changed. In making decisions about anticoagulant choice in CAVT, providers are likely influenced by a number of factors including the results from clinical trials of DOACs in CAVT, although in our Health System a trend in increased DOAC utilization in CAVT began long before such clinical trial results were reported. Despite increased use of DOACs in CAVT, providers continue to feel most comfortable with enoxaparin, which remains the most commonly used anticoagulant in CAVT. Further prospective real-world data are needed to assess providers' prescribing factors, cost, and utilization patterns of DOACs in CAVT, and to assess how such practices impact bleeding and re-thrombosis rates.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal