

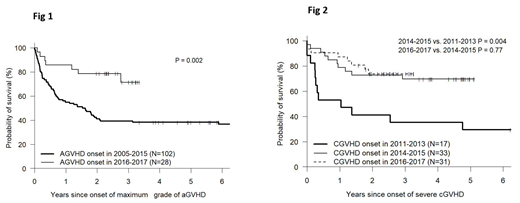
Severe (grade 3-4) acute GVHD (aGVHD) and NIH grade severe chronic GVHD (cGVHD) have historically been associated with poor survival. However, earlier diagnosis, improved treatment and supportive care, may result in an improvement in outcomes for patients recently diagnosed with severe GVHD compared to prior cohorts. Our institution has prospectively documented onset, grading and therapy of patients with GVHD using a single dedicated practitioner since 2005. We assessed 851 consecutive patients who received allografts at our center between 1/2005 and 12/ 2016 and identified 130 patients (15.3%) who developed severe aGVHD through Dec 2017 without prior relapse of malignancy. Characteristics were: median age 52.5, 51% male, race-81% white -17% black, diagnosis- AML 31% - MDS/MPD 20%- NHL/HL/CLL-23%, -ALL 11%, donor - MRD 21% - MUD 49% - haplo 30%, PBSC 78%, BM 17%, CBU 5%, preparative regimen MAC 44% - RIC/NST 56%, median time from BMT to onset of severe aGVHD was 49 days (7-376). Maximum grade = gd 3 (85%), gd 4 (15%), Median follow-up for survivors from date of onset was 59 months (23-155m). Survival estimates for the entire cohort from date of onset of grade 3-4 aGVHD at 1, 2 and 3 years were 62%, 49% and 47% respectively. Patients who developed severe aGVHD in 2016-2017 had significantly improved overall survival compared to patients who developed severe acute GVHD in prior years (2005-2015) -1 and 2 yr survival 86% & 79% vs 55% & 41% respectively, p=0.002 log-rank test, Fig 1). No significant differences were found between earlier cohorts. On multivariable analysis assessing the following variables: age, gender, race, diagnosis, donor type, cell source, regimen intensity, DRI, HCT-CI, CMV status, grade of aGVHD (3 vs 4), days from transplant to gd 3-4 aGVHD onset, year of development of severe acute GVHD (2016-2017 vs earlier) remained significant for survival (HR 0.36, p=0.018). Other significant variables were grade 4 vs 3 GVHD (HR 3.78, p<0.001) and DRI (high/very high vs low/intermediate, HR 1.84, p=0.011).
For cGVHD we assessed 522 consecutive patients who underwent allografts between 4/2011 (start date of prospective documentation of NIH grade cGVHD )and 12/2016, and identified 146 (28%) patients who developed moderate to severe NIH grade chronic GVHD without prior relapse by Dec 2017 (85 severe, 61 moderate). Patient characteristics were: median age 53, 55% male, race-74% white -22% black, AML 40% - MDS/MPD 31%- NHL/HL/CLL-15%, -ALL 12% , donor - MRD 34% - MUD 40% - haplo 25%, graft- PBSC 82%, BM 18%, preparative regimen MAC 54% - RIC/NST 44%, median time from BMT to onset of moderate/severe cGVHD was 289 days (27-1364). Median follow-up for survivors from date of onset of moderate to severe GVHD was 48 months (19-94m). Estimated rates of survival from date of onset of moderate to severe cGVHD for the entire cohort at 1, 2 and 3 years were 82%, 73% and 71% respectively. For patients who developed severe cGVHD the corresponding survival estimates were 77%, 67% and 63%. No significant difference in post-onset survival was encountered when comparing patients developing moderate cGVHD in 2011-2013, 2014-2015 and 2016-2017. However, for severe cGVHD, 1 and 2 year estimated survival rates for the three cohorts were : 53% & 41%, 79% & 73% and 87% and 74% respectively (p=0.004 for 2011-2013 vs 2014-2015 but p=NS for 2014-2015 vs 2016-2017, Fig 2). On a multivariable analysis considering age, gender, race, diagnosis, donor type, graft source, regimen intensity, DRI, HCT-CI, and days from transplant to cGVHD onset, none of these variables was significantly associated with post-cGVHD survival. In the Cox model including year of onset of severe cGVHD, onset in recent years was linked to lower risk of mortality compared to onset in earlier years (onset 2014-2015 vs 2011-2013 - HR=0.34, p-0.012; onset 2016-2017 vs 2011-2013 - HR=0.28, p=0.006). These data suggest that survival of patients developing either severe aGVHD or severe NIH grade cGVHD has significantly improved in recent years compared to historical controls. More than two-thirds of such patients now survive two years from onset of severe GVHD. This must be taken into account when evaluating novel therapies for severe GVHD.
Solh:ADC Therapeutics: Research Funding; Celgene: Speakers Bureau; Amgen: Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal