

Background & Purpose: Gut graft-versus-host disease (GVHD) is a serious complication after hematopoietic stem cell transplantation (HSCT) and is associated with high mortality. Mucosal-associated invariant T cells (MAIT) are a group of innate-like T cells enriched in the intestine, which may alter the composition of the intestinal microflora or exert a certain immunomodulatory effect to protect the intestinal mucosa from further damage for the inflammatory response. However, little is known about the regulatory role of MAIT cells in development and progression of gut GVHD. Infused MAIT in grafts will facilitate the reconstruction of MAIT after transplantation. Thus, we aimed to investigate the correlation between the number of MAIT cells in the graft and the occurrence of gut GVHD.
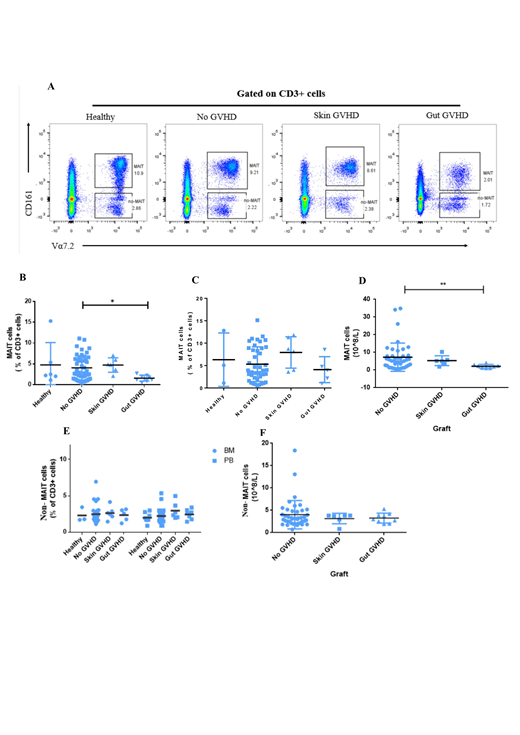
Methods & Cases: Our transplantation setting used the graft composed of bone marrow stem cells (BMSC) and peripheral blood stem cell (PBSC). We prospectively studied 60 patients undergoing allo-HSCT and 9 healthy donors in our institute. In our study, the number of MAIT cells in the graft was evaluated by multiparameter flow cytometry (FCM). MAIT cells were defined as a group of cells expressing CD3+CD161hiVa7.2+. To better compare the specific changes in the number of MAIT cells in the graft in groups of healthy donors, no GVHD patients, skin GVHD patients, and gut GVHD patients, we chose a group of non-MAIT cells that express CD3+CD161-Va7.2+ as a reference(Fig.1A). We compared the number and frequency of MAIT and non-MAIT cells in the 4 groups.
Results: In the 60 transplanted patients, 9 patients developed into gut GVHD and 6 patients developed into skin GVHD. In patients with gut GVHD, the frequency of MAIT cells in the graft of PBSC was lower compared to that of no GVHD (No GVHD vs. gut GVHD, P=0.045. Fig.1B), but no difference was detected in the graft of BMSC among these groups (No GVHD vs. gut GVHD, P=0.191; Healthy vs. gut GVHD, P=0.298; Skin GVHD vs. gut GVHD, P=0.071. Fig.1C). The total number of infused MAITs in the graft of gut GVHD patients was significantly lower than that of no GVHD and skin GVHD patients (no GVHD vs. gut-GVHD, P=0.001. Fig.1D). In addition, the frequency and number of MAIT cells in the graft were not different between no GVHD and skin GVHD patients (P>0.05, Fig.1B, C and D). Finally, in the graft of patients with no GVHD, skin GVHD and gut GVHD, the difference in the frequency and number of non-MAIT cells was not significant (all P>0.05, Fig.1E and Fig.1F).
Conclusions: In conclusion, gut GVHD was more likely to occur in patients who were infused with a smaller number of MAIT cells in grafts. In addition, the number of MAIT cells in the graft had no significant correlation with the occurrence of skin GVHD. These results suggested the potential functional effects of MAIT cells on gut GVHD. However, the specific biological role of MAIT cells in maintaining the homeostasis of intestinal tract and how MAIT cells would influence the onset of gut GVHD are still unclear. It may function through direct immunosuppression or regulation of intestinal microflora, which needs to be confirmed by further mechanical studies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal