

Karl S Peggs and Sarah J Albon contributed equally to the work and are joint first author
Introduction
Alemtuzumab reduces the incidence of GVHD after unrelated donor stem cell transplant (MUD SCT) but delays immune reconstitution resulting in high morbidity/mortality from viral infections. Previous studies have suggested that adoptive transfer of allodepleted donor T cells (ADTs) improves immunity after SCT but this has never been tested in a randomised study. We developed a methodology for selective immunomagnetic depletion of alloreactive T-cells upregulating CD25 and CD71 after activation with host dendritic cells (DC) and showed that ADTs retain anti-viral responses with minimal host alloreactivity (Samarasinghe et al Blood 2010). We have now tested whether ADTs can safely be used to improve immune reconstitution after MUD SCT for haematological malignancies in a randomised Phase II multi-centre clinical study; ICAT (NCT01827579).
Methods
Patients undergoing Alemtuzumab-based peripheral blood SCT from a 9/10 or 10/10 MUD for haematological malignancy were randomised 2:1 to receive either the ATIMP (ADTs) or standard of care. Two weeks prior to SCT, patients randomised to ATIMP underwent a leucapheresis from which DCs were generated. Irradiated patient-derived DCs were then co-cultured with peripheral blood mononuclear cells (PBMC) from an unstimulated leucapheresis/500ml blood draw from the donor to activate alloreactive T cells. Four days later, the co-culture was depleted of CD25+ and CD71+ fractions by immunomagnetic depletion on the CliniMACs, sampled for residual alloreactivity and sterility, and cryopreserved. Patients randomised to the ATIMP were scheduled to receive 3 escalating doses of ADTs (0.1x106/Kg at day 30, 0.3x106/Kg at day 60 and 1x106/Kg at day 90 post-SCT) until either there was >grade 1 aGVHD or they had normal circulating T cells (>700/µL). The primary end-point of the study was circulating CD3+ T cell count at 4 months post-SCT with one-sided 15% significance level. Acute/chronic GVHD were graded using the Seattle/NIH criteria respectively.
Results
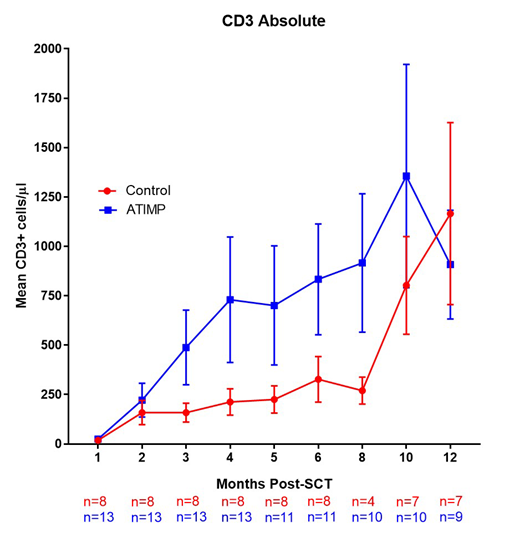
Twenty one patients were treated, 13 on the ATIMP arm and 8 on the control arm. The median age was 53 years and 67% (14) were male. 12 were AML/Myelodysplasia, 5 NHL, 3 CLL/CML and 1 HL. The median follow-up time is 14 months. Five of 13 ATIMP patients received 1 dose of ADTs, 4/13 2 doses and 4/13 all 3 doses. The incidence of acute and chronic GVHD was comparable between the arms. Overall, 7/13 ATIMP patients developed significant (>Grade 2) acute GVHD compared to 4/8 of the control arm (p>0.99). 3/13 patients in the ATIMP arm and 2/8 patients in the control arm developed severe aGVHD (all Grade 3). Three of 13 ATIMP cohort patients developed chronic GVHD (1 mild, 1 moderate, 1 severe), compared to 3/8 (all mild) in the control cohort. At 4 months, the circulating CD3+ T cell count mean was 730/µL (range 10-4080) in the ATIMP group and 212.5/µL (range 10-500) in the control group (1-sided p=0.11). However, the data was not normally distributed (Wilcoxon 1-sided p=0.18). Three ATIMP patients had high CD3+ T cell count at 4 months (>1000/µL). At 6 months, the mean circulating CD3+ T cell count was 833.6/µL (range 20-2690) and 327.5/µL (range 10-860). At month 4, the mean PHA stimulation index in the ATIMP arm was 16.8 (range 0.67- 73.1) vs 3.8 (range 1.1-8.2) in the control group. At 4 and 6 months post-SCT, spectratyping analysis showed no evidence of a difference in Vβ diversity between the 2 arms in both CD4+ and CD8+ cells. The 1-year survival rate in the ATIMP cohort is 92% vs 88% in the control, and 1-year disease free survival rate 67% in the ATIMP cohort vs 70% in the control.
Conclusions
These data suggest that adoptive transfer of ADTs improves T cell reconstitution in some patients after MUD SCT and that the GVHD rates were similar between ATIMP and control groups.
Figure 1: Kinetics of T cell recovery after transplant in ATIMP (blue) and Control (red) patients. Mean +/- SEM shown.
Peggs:Gilead: Consultancy, Speakers Bureau; Autolus: Membership on an entity's Board of Directors or advisory committees. Ghorashian:UCLB: Patents & Royalties: UCLB; Celgene: Honoraria; novartis: Honoraria. Amrolia:UCLB: Patents & Royalties.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal