

Background
Human herpesvirus-6 (HHV-6) encephalitis occurs frequently through cord blood transplantation (CBT), and leads to a high risk of mortality and morbidity. Although CBT is a known risk factor for HHV-6 encephalitis, a thorough analysis of risk factors for HHV-6 encephalitis in patients receiving CBT has not been performed, and several risk factors remain unidentified. In our center, generally, either tacrolimus (Tac) plus methotrexate (MTX) (Tac/MTX) or mycophenolate mofetil (MMF) (Tac/MMF) was selected for graft-versus-host disease (GVHD) prophylaxis after CBT, at the physician's discretion. However, in recent years, Tac/MMF became the standard choice. We observed that the incidence of HHV-6 encephalitis tended to be markedly higher among patients receiving treatment with a cyclophosphamide (Cy) and total body irradiation (TBI) (Cy/TBI)-based regimen and Tac/MMF after CBT. Therefore, we aimed to ascertain whether certain conditioning regimens and GVHD prophylaxis regimens are associated with the occurrence of HHV-6 encephalitis after CBT.
Methods
In this retrospective study, we examined 103 patients undergoing CBT for hematological diseases at our center between 2011 and 2019. To analyze the effect of GVHD prophylaxis on the occurrence of HHV-6 encephalitis, we divided patients into two groups based on the GVHD prophylaxis regimen used: the Tac/MTX group and the Tac/MMF group. We excluded one patient who received Tac alone and one who received cyclosporine plus MTX. Finally, 101 patients were enrolled. Routine peripheral blood examinations for HHV-6 were performed once or twice a week. HHV-6 encephalitis was defined as the presence of a central nervous system dysfunction, along with a positive polymerase chain reaction result for HHV-6 DNA in the cerebrospinal fluid. HHV-6 viremia was defined as the presence of HHV-6 in the peripheral blood.
Results
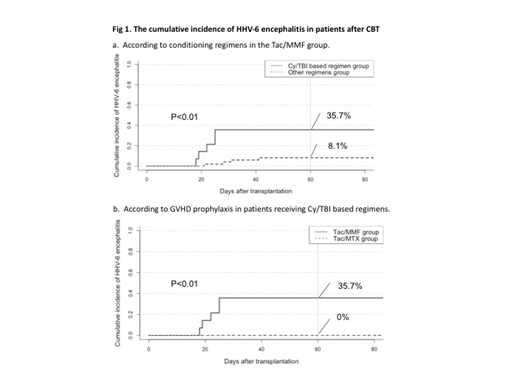
The median age of patients was 47 years, and the median follow-up duration for surviving patients was 432 days. Conditioning regimens included myeloablative conditioning (MAC, n=64) and reduced-intensity conditioning (RIC, n=37). MAC included Cy/TBI-based regimens in 42 patients and fludarabine (Flu) plus busulfan (Bu) (Flu/Bu)-based regimens in 23, and RIC included Flu plus melphalan-based regimens in 34 patients and other regimens in 2. Sixty-four patients received Tac/MMF as GVHD prophylaxis, whereas 37 received Tac/MTX. Six patients received HLA-matched (6/6) cord blood (CB), 27 received HLA one-antigen mismatched CB, and 68 received HLA two-antigen mismatched CB. The median total nucleated cell number and CD34-positive cell number at cryopreservation were 2.2 × 107/kg and 0.7 × 105/kg, respectively. Thirteen patients (12.8%) experienced primary graft failure. Overall, the cumulative incidence of HHV-6 viremia on day 40 was 68%, and the median time from CBT to HHV-6 viremia was 23 days. The cumulative incidence of HHV-6 viremia was significantly higher in the Tac/MMF group than in the Tac/MTX group (Tac/MMF group, 75%; Tac/MTX group, 56%; p=0.03). Ten patients developed HHV-6 encephalitis. Overall, the cumulative incidence of HHV-6 encephalitis on day 60 was 10.1%. The cumulative incidence of HHV-6 encephalitis tended to be higher in the Tac/MMF group than in the Tac/MTX group (14.1% vs. 2.7%, respectively; p=0.08). Therefore, the administration of Tac/MMF as GVHD prophylaxis after CBT was identified as a probable risk factor for HHV-6 encephalitis, and we sought to identify more such risk factors, specifically among patients receiving Tac/MMF. In the analysis of Tac/MMF group, the cumulative incidence of HHV-6 encephalitis was significantly higher among patients receiving Cy/TBI-based regimens than among those receiving other regimens (35.7% vs. 8.1%, respectively; p<0.01) (Fig. 1a). In addition, among the entire group of patients receiving Cy/TBI-based regimens, the cumulative incidence of HHV-6 encephalitis was significantly higher in the Tac/MMF than in the Tac/MTX group (35.7% vs. 0%, respectively; p<0.01) (Fig. 1b).
Conclusion
Our analysis showed that patients receiving Tac/MMF as GVHD prophylaxis after CBT with a Cy/TBI-based regimen have a significantly higher risk of developing HHV-6 encephalitis. Further studies using a large cohort are required to elucidate the association between the occurrence of HHV-6 encephalitis and the use of Tac/MMF in patients undergoing CBT with a Cy/TBI-based regimen.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal