

Background
Deregulation of histone acetylation has been recognized to serve a critical role in the pathogenesis of multiple myeloma (MM), which histone deacetylase (HDACs) are overexpressed in plasma cells derived from patients with MM. Therefore, HDACs may promise targets for MM therapy, and panobinostat was approved by the FDA for the treatment of relapsed/refractory MM in 2015. Chidamide, a novel oral benzamide type HDAC inhibitor independently developed in China and approved as peripheral T-cell lymphoma, selectively suppresses the activity of class I HDACs. Studies have shown that chidamide can enhance cytotoxic effect of bortezomib or lenalidomide on MM cells in vitro, which suggested a synergistic combination of chidamide with bortezomib or lenalidomide at a low dose. This Phase I clinical trial was designed to investigate the efficacy and safety of dose-escalating chidamide with VRD as induction chemotherapy for newly-diagnosed high-risk multiple myeloma (MM) patients before autologous transplantation (NCT 04025450).
Methods
The de novo MM patients who had any one of the followings was defined as high-risk MM: a. high-risk cytogenetics including 17p-, t (4, 14), t (14, 16), t (14, 20), 1q gain, 1p-, double hit myeloma, triple hit myeloma. b. R-ISS stage III. c. IgD/IgE type. d. with measurable extra-medullary plasmacytoma. e. peripheral blood clonal plasma cell≥0.165% by 10-colour flow cytometry. Chidamide at 4 dose levels (15mg/20mg/25mg/30mg d0,3,7,10) were administered to 12 patients with VRD (bortezomib 1.3mg/m2 d1,4,8,11, lenalidomide 25mg d1-14, and dexamethasone 20mg/d d1-2,4-5,8-9,11-12), every 21 days for 4-cycle induction therapy. Safety, DLT and efficacy of Chi-VRD were observed. Pain sore before each cycle and the whole body DWI-MR before and after 4-cycles were done to see whether improvement in osteodynia and sclerotin reparation of patients. All patients will be collected autologous stem cell to see whether there is effect of the regimen on stem cells after 4-cycle induction therapy.
Results
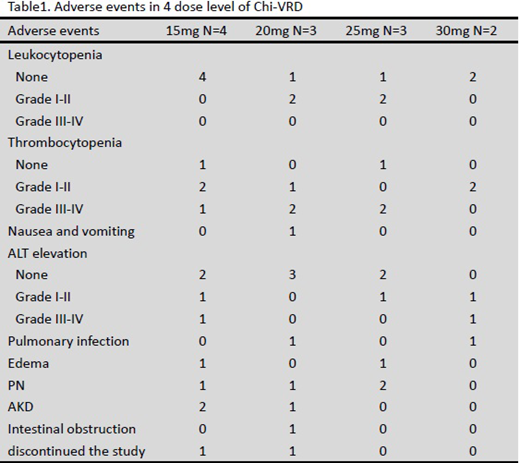
The median age of these 12 patients was 57.5 (45, 65), 50.0% was male and 25% (3/12) patients had renal insufficiency with creatinine≥177umol/l or Ccr≤40ml/min. 2 patients were R-ISS stage III; 4 had measurable extra-medullary plasmacytoma; 7 had circulating plasma cells ≥0.165%; and one had t(4;14). The total adverse events were listed in the table below (table1). The main treatment-related adverse events were hematological toxicity, hepatotoxicity, edema, deterioration of renal function and heart failure. Two patients with renal insufficiency had to stop this induction therapy, one for serious adverse event of acute heart failure and acute renal failure at the first cycle in the 20mg dose group and another one for intermittent medication in the 15mg group. All patients had osteodynia relief. Among the 9 patients who have had response evaluation, the ORR was 100% and 77.8% (7/9) patients had gotten very good partial response (VGPR) or better after one cycle.
Conclusion
This was the first report of ChiVRD induction treatment for newly diagnosed high risk MM. The preliminary results of Chi-VRD suggested excellent efficacy with rapid response. The most common adverse events were hematological toxicity and hepatotoxicity. No dose limiting toxicity (DLT) was observed at 4 dose levels. Hematological toxicity and hepatotoxicity may increase with the dosage increase, but could be quickly controlled. Although chidamide does not affect renal function itself, patients with renal insufficiency may have more adverse reactions that may need dose adjustment. Updated results with comparison between VRD and Chi-VRD will be presented at the following phase II trial.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal