

Introduction
UK and Ireland clinicians gained non-trial access to ibrutinib for relapsed / refractory CLL through a named patient scheme (NPS) for 7 months in 2014, and the UK CLL Forum has been following a cohort of 315 NPS patients treated with ibrutinib at 66 UK and Ireland hospitals. We now update this dataset with up to 5 years follow-up.
Results
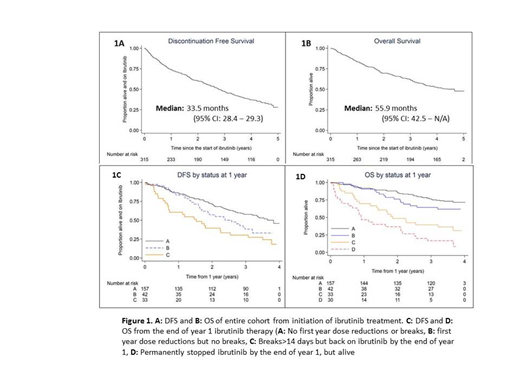
The primary end-points of the study were Discontinuation Free Survival (DFS) and Overall Survival (OS). Of the original 315 patients, 213 have stopped ibrutinib and 159 patients have died, with all living patients having a survival update in 2019. With 55.6 months median follow-up, median DFS was 33.5 months (95% CI: 28.4-29.3) and median OS was 55.9 months (95% CI: 42.5-N/A) (Figure 1A and 1B). Four years after starting ibrutinib, 37.0% of patients were still taking ibrutinib and 52.4% were still alive.
Both DFS and OS were inferior for older (age > median) and PS 2+ patients. Patients with 17p- have inferior DFS and OS compared to patients with other defined cytogenetic aberrations (13q-, 11q-, t(12)) and more patients with 17p- compared with non-17p- stopped ibrutinib for progressive CLL (PD) (26.4% vs 18.8%; p=0.01) and Richter's Syndrome (12.1% vs 8.3%; p=0.05). First relapse patients had more than a 3 fold lower rate of ibrutinib discontinuation due to CLL progression (7.1% versus 24.5%; two-tailed Fisher's exact test; p=0.001) compared with patients receiving ibrutinib at later lines of therapy, although DFS and OS for these groups were similar. With multivariable analysis of pre-treatment factors, older age, PS2+, 17p- and >1 prior line of therapy retained significance for earlier ibrutinib discontinuation and age, PS2+ and 17p- associated with inferior OS.
To analyze any potential impact of reduced ibrutinib dosing during the first year of therapy, we originally classified all patients alive at 12 months into 4 groups, depending on first-year ibrutinib treatment. Group A: No dose reductions or breaks >14 days; Group B: Dose reductions, but no breaks > 14 days; Group C: Breaks > 14 days but back on ibrutinib by 1 year; Group D: stopped ibrutinib permanently but still alive at 1 year. With extended follow-up, patients dose reduced in year 1 are very likely to have on-going dose reductions beyond the first year (86% patients in group B are still dose reduced beyond 4 years, compared with 12% in group A). Groups A and B retain similar DFS and OS initially, although beyond 2 years the curves separate (Figure 1C and 1D) (DFS HR: 1.62 (1.05-2.50), OS HR: 1.52 (0.86-2.70)). Interestingly, the dose-reduced group do not have a higher incidence of disease progression, (PD A:24.8%, PD B:23.8%), but have a higher chance of discontinuation for all non-PD causes (A:23.6%, B:42.9%). With longer follow-up, patients from groups C and D had significantly impaired OS compared with group A, with 4 year OS 39.4% and 16.7% respectively compared with 76.4% for group A (p<0.001).
Considering all patients who discontinued ibrutinib, stopping for AEs decreased over time (year 1: 57%, 2: 53%, 3: 30%, 4: 21%). Stopping for infection was much more common in the first year (19.5%) compared with years 2 to 4 (8.4%). The risk of stopping ibrutinib due to PD-CLL increases with time (year 1: 11%, 2: 18.6%, 3: 42.5%, 4: 57.6%). Of the PD-CLL patients, treatment with venetoclax had the best OS (n=43; 1 year OS: 77.5%) compared with the 7 treated with rituximab / idelalisib (1 year OS: 42.9%) and 14 treated with other strategies (including palliative care) (1 year OS: 10%). Although this supports the use of venetoclax for disease progression post ibrutinib, there are two potentially significant biases; more palliative patients did not receive venetoclax and patients who relapsed within 1 year of starting ibrutinib, who were potentially more unstable biologically, did not receive venetoclax (unavailable in the UK pre-2016)
Conclusions
With approaching 5 years of follow-up, around one third of 'real-world' UK / Ireland patients treated with ibrutinib for relapsed / refractory CLL remain on ibrutinib. Our data suggest that younger, better performance status patients who have had fewer prior lines of therapy and no evidence of 17p deletion seem most likely to remain on ibrutinib long-term. Likewise, patients who remain free of adverse events that often associate with dose reductions and treatment breaks, have the best chances of remaining on ibrutinib. Treatment of PD-CLL with venetoclax post ibrutinib shows encouraging results.
CLL Forum:Roche: Other: Sponsorship of the UK CLL Forum; Abbvie: Other: Sponsorship of the UK CLL Forum; Janssen: Other: Sponsorship of the UK CLL Forum; Gilead: Other: Sponsorship of the UK CLL Forum. Follows:Janssen: Consultancy, Honoraria, Speakers Bureau; Abbvie: Consultancy, Honoraria, Speakers Bureau; Roche: Consultancy, Honoraria, Speakers Bureau; AZ: Consultancy, Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal