

Background: The Antibody-Coupled T-cell Receptor (ACTR) platform is an autologous engineered T-cell therapy that combines the cell-killing ability of T cells and the tumor-targeting ability of co-administered antibodies to exert potent antitumor immune responses. ACTR707 comprises the extracellular domain of CD16 linked to a CD3ζ signaling domain and a CD28 co-stimulatory domain. ACTR707 is in clinical development in combination with rituximab (NCT03189836) or trastuzumab (NCT03680560).
Here we present clinical findings from the dose escalation phase of Study ATTCK-20-03, an ongoing, multicenter, phase 1 study of ACTR707+rituximab in subjects with relapsed or refractory (R/R) CD20+ NHL.
Methods: The primary objectives of this first-in-human study are to evaluate the safety of the combination of ACTR707 and rituximab and to determine a recommended phase 2 dose (RP2D). Other objectives include evaluating antitumor activity and ACTR T-cell persistence. Subjects must have CD20+ NHL that is R/R after prior treatments, which must include anti-CD20 antibody-containing chemotherapy. Subjects receive lymphodepleting chemotherapy (cyclophosphamide and fludarabine) for 3 days, followed by rituximab and a single dose of ACTR707. Additional doses of rituximab are administered q3w until disease progression, unacceptable toxicity, or Investigator decision. The study includes a dose escalation phase (increasing doses of ACTR707 with fixed dose of rituximab at 375 mg/m2 q3w) and an expansion phase at the RP2D.
Results: Six subjects received ACTR707 at Dose Level 1 (DL1; 23-38×106 ACTR+ T cells), 3 subjects at DL2 (30-50×106 ACTR+ T cells), and 5 subjects at DL3 (45-55×106 ACTR+ T cells). The majority of the subjects were diagnosed with DLBCL (93%) and had refractory disease (71%), defined as progressive disease as the best response to any prior treatment or relapse <1 year post autologous stem cell transplant.
In DL1 through DL3, as of 27 May 2019, there were no dose-limiting toxicities, AEs of cytokine release syndrome (CRS), serious or severe neurologic AEs, or AEs leading to deaths on treatment. TEAEs reported in >2 subjects, regardless of causality or grade, included neutropenia, thrombocytopenia, anemia, febrile neutropenia, pyrexia, cough, constipation, diarrhea, nausea, and vomiting. SAEs considered possibly related to ACTR707 were febrile neutropenia (n=2) and cytopenia (n=1).
ACTR707 expansion generally reached peak levels within 1 to 2 weeks after administration. All subjects with complete response (CR) up to 1 year had detectable ACTR at the last timepoint evaluated. Higher ACTR707 CD8:CD4 T-cell ratios were associated with clinical responses.
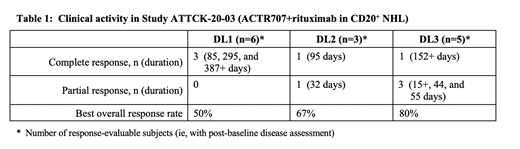
Clinical activity was reported across DL1 through DL3, with an overall response rate of 64% including durable complete responses (CRs), with one subject in CR for 387+ days (Table 1).
Conclusions: Data available from DL1 through DL3 of ACTR707+rituximab suggest that clinical responses can be achieved without severe T cell-mediated toxicities (eg, CRS and neurotoxicity) that have been reported with other autologous T-cell products. Dose escalation continues at a target dose of 80×106 ACTR+ T cells; enrollment in DL4 (n=6) was recently completed. Updated data, including identified correlates of clinical outcomes, will be presented for DL1 through DL4.
Flinn:TG Therapeutics, Trillum Therapeutics, Abbvie, ArQule, BeiGene, Curis, FORMA Therapeutics, Forty Seven, Merck, Pfizer, Takeda, Teva, Verastem, Gilead Sciences, Astra Zeneca (AZ), Juno Therapeutics, UnumTherapeutics, MorphoSys, AG: Research Funding; AbbVie, Seattle Genetics, TG Therapeutics, Verastem: Consultancy; TG Therapeutics, Trillum Therapeutics, Abbvie, ArQule, BeiGene, Curis, FORMA Therapeutics, Forty Seven, Merck, Pfizer, Takeda, Teva, Verastem, Gilead Sciences, Astra Zeneca (AZ), Juno Therapeutics, UnumTherapeutics, MorphoSys, AG: Research Funding; Acerta Pharma, Agios, Calithera Biosciences, Celgene, Constellation Pharmaceuticals, Genentech, Gilead Sciences, Incyte, Infinity Pharmaceuticals, Janssen, Karyopharm Therapeutics, Kite Pharma, Novartis, Pharmacyclics, Portola Pharmaceuticals: Research Funding; F. Hoffmann-La Roche Ltd: Research Funding. Westin:Genentech: Other: Advisory Board, Research Funding; Janssen: Other: Advisory Board, Research Funding; Kite: Other: Advisory Board, Research Funding; Unum: Research Funding; Curis: Other: Advisory Board, Research Funding; Juno: Other: Advisory Board; MorphoSys: Other: Advisory Board; 47 Inc: Research Funding; Celgene: Other: Advisory Board, Research Funding; Novartis: Other: Advisory Board, Research Funding. Cohen:Genentech, Inc.: Consultancy, Research Funding; Takeda Pharmaceuticals North America, Inc.: Research Funding; Gilead/Kite: Consultancy; LAM Therapeutics: Research Funding; UNUM: Research Funding; Hutchison: Research Funding; Astra Zeneca: Research Funding; Lymphoma Research Foundation: Research Funding; ASH: Research Funding; Bristol-Meyers Squibb Company: Research Funding; Seattle Genetics, Inc.: Consultancy, Research Funding; Janssen Pharmaceuticals: Consultancy. Akard:Celgene: Speakers Bureau; Novartis: Speakers Bureau; Takeda: Speakers Bureau; Bristol-Myers Squibb: Speakers Bureau; Gilead: Speakers Bureau. Jaglowski:Juno: Consultancy, Other: advisory board; Kite: Consultancy, Other: advisory board, Research Funding; Unum Therapeutics Inc.: Research Funding; Novartis: Consultancy, Other: advisory board, Research Funding. Sachs:Unum Therapeutics Inc.: Employment. Ranger:Unum Therapeutics Inc.: Employment. Harris:Unum Therapeutics Inc.: Employment. Payumo:Unum Therapeutics Inc.: Employment. Bachanova:Celgene: Research Funding; Gamida Cell: Research Funding; Seattle Genetics: Membership on an entity's Board of Directors or advisory committees; GT Biopharma: Research Funding; Kite: Membership on an entity's Board of Directors or advisory committees; Incyte: Research Funding; Novartis: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal