


Background/Objectives
Infants with ALL have poor outcomes, especially the 70-80% with KMT2A rearrangements (KMT2A-r). Intensification of chemotherapy has reached the limit of tolerability, and stem cell transplantation (SCT) has not improved outcomes. The FLT3 kinase is overexpressed and constitutively activated in KMT2A-r ALL. FLT3 inhibitors (FLT3i) selectively kill KMT2A-r ALL cells in vitro and in vivo, and synergize with chemotherapy. COG AALL0631 was a randomized trial that tested the hypothesis that the addition of the FLT3i lestaurtinib to post-induction chemotherapy would improve outcomes for KMT2A-r ALL.As previously reported, the addition of lestaurtinib did not improve outcomes [3-year disease-free/overall survival (DFS/OS) 39%/46% without lestaurtinib vs. 37%/45% with lestaurtinib, log-rank p=0.78/0.92]. We hypothesized that correlative laboratory measures of FLT3i pharmacodynamics and ex vivo FLT3i sensitivity would enhance our understanding of the clinical responses for KMT2A-r infants treated with lestaurtinib.
Design/Methods
FLT3i pharmacodynamics (PD) were determined using plasma inhibitory activity (PIA) measured at 5 trough time points during lestaurtinib treatment, using Western blotting and densitometry (normalized to pre-treatment levels). PIA ranged from 0% (no evidence of FLT3 inhibition) to 100% (full inhibition). Mean PIA of 5 troughs was calculated for each patient, and was categorized based on pre-defined protocol criteria as "adequate", or FLT3 inhibited (≥85%) vs "inadequate", or FLT3 uninhibited (<85%). FLT3i ex-vivo sensitivity (EVS) was determined using WST-1 cell proliferation assay [48 hour cytotoxicity of diagnostic blasts exposed to 50 nM lestaurtinib vs vehicle control; mean of triplicate wells; ranging from 0% (no cytotoxicity) to 100% (all cells killed)]. Median cytotoxicity was calculated for all assayed samples on the trial (n=151; median cytotoxicity 46%). Samples were categorized as "sensitive" (above median) or "resistant" (below median). Clinical outcomes examined included 3-year DFS and OS (measured from randomization) and minimal residual disease (MRD) measured in a central laboratory by flow cytometry at week 10 [after induction (6 weeks) followed by chemotherapy vs. chemotherapy/lestaurtinib intensification (4 weeks)]. MRD results were categorized as negative (<0.01%) or positive (≥0.01%). P-values for DFS and OS comparisons are based on log-rank test, and for MRD comparisons are based on Fisher's exact test.
Results
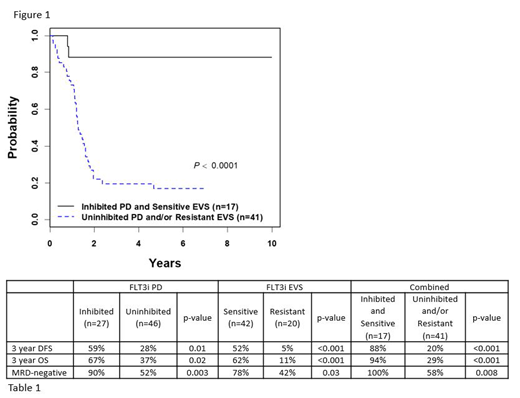
Of 210 eligible patients, 146 were KMT2A-r, and 78 were assigned to receive lestaurtinib. Of these, data were available for FLT3i PD (n=73), FLT3i EVS (n=62), MRD (n=55), and DFS/OS (n=78). FLT3i PD and FLT3i EVS significantly correlated with both survival and MRD. For FLT3i PD, 27 were "FLT3 inhibited" and 46 were "FLT3 uninhibited". The DFS/OS for inhibited was 59%/67% vs. 28%/37% for uninhibited (p=0.01/0.02). The week 10 MRD-negative rate was 90% for inhibited vs. 52% for uninhibited (p=0.003). For FLT3i EVS, of the 62 lestaurtinib-treated patients with data, 42 were "sensitive" and 20 were "resistant". The DFS/OS for sensitive was 52%/62% vs. 5%/11% for resistant (p<0.001 for both). The week 10 MRD-negative rate was 78% for sensitive vs. 42% for resistant (p=0.03). We then hypothesized that among patients treated with lestaurtinib, those with both "inhibited" FLT3i PD and "sensitive" FLT3i EVS would have particularly good clinical outcomes. Of 58 patients with data for both assays, 17 were both inhibited and sensitive. This cohort had DFS/OS of 88%/94% and week 10 MRD-negative rate of 100%. The remaining N=41 were uninhibited and/or resistant, and had DFS/OS of 20%/29% (p<0.001 for both, Figure 1 shows DFS) and week 10 MRD-negative rate of 58% (p=0.008). Table 1 summarizes all results.
Conclusion
While the addition of lestaurtinib to chemotherapy did not improve outcomes, patients achieving potent pharmacodynamic inhibition of FLT3 and those whose leukemia cells were sensitive to ex-vivo FLT3-inhibitor induced cytotoxicity did benefit from the addition of lestaurtinib. Selection of patients with FLT3-sensitive leukemia, real-time intra-patient dose escalation of patients with inadequate pharmacodynamics, and/or using a more potent FLT3 inhibitor may enhance the efficacy of FLT3 inhibition for KMT2A-r infant ALL.
Raetz:Pfizer: Research Funding. Loh:Medisix Therapeutics, Inc.: Membership on an entity's Board of Directors or advisory committees. Hunger:Bristol Myers Squibb: Consultancy; Amgen: Consultancy, Equity Ownership; Novartis: Consultancy; Jazz: Honoraria. Borowitz:Beckman Coulter: Honoraria. Small:Pharos I, B & T: Consultancy, Research Funding; InSilico Medicine: Membership on an entity's Board of Directors or advisory committees.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal