

Background:
The availability of factor (F)VIII replacement products has dramatically improved life expectancy for patients with hemophilia A (HA). However, older patients face distinct challenges. Age-related comorbidities such as cardiovascular disease (CVD), often involving treatments that can increase the risk of bleeding, and patients who received treatment before the advent of recombinant products, are more likely to have been exposed to blood-borne viruses carrying chronic infections. It is important to understand clinical outcomes with FVIII products in patients with HA and these comorbidities.
BAY 94-9027 (damoctocog alfa pegol; Jivi) is a B-domain deleted recombinant FVIII, site-specifically PEGylated with a 60 kDa (2×30 kDa) polyethylene glycol to extend its half-life. Efficacy and safety of BAY 94-9027 as prophylactic and on-demand therapy for patients with severe HA were demonstrated in the phase II/III PROTECT VIII trial and its Extension.
This post hoc analysis assessed bleeding rates and safety outcomes for prophylaxis patients in PROTECT VIII and its Extension, based on the presence or absence of comorbidities of interest.
Patients/Methods:
PROTECT VIII (NCT01580293) was a partially randomized, open-label trial of 134 males aged 12-65 years with severe HA (FVIII <1%) and ≥150 FVIII exposure days. Prophylaxis patients (n=114) received BAY 94-9027 25 IU/kg twice weekly (2×W) for a 10-week run-in period. Patients with ≤1 spontaneous joint or muscle bleed during this period were randomized to 45-60 IU/kg every 5 days or 60 IU/kg every 7 days for the main 26-week study; patients enrolling after the randomization arms were full, or with ≥2 bleeds in the run-in period, received 30-40 IU/kg 2×W. Patients completing the main study could enter an extension, continuing BAY 94-9027 on any regimen used in the main study.
Baseline characteristics, annualized bleeding rates (ABR) and safety were examined for patients on prophylaxis treatment during main study and its Extension with and without comorbidities of interest. Comorbidities included human immunodeficiency virus (HIV) infection, hepatitis B or C infection (HBV or HCV), and risk factors for CVD (hypertension, hypercholesterolemia, hypertriglyceridemia and hyperlipidemia).
Results:
A total of 104 patients who received BAY 94-9027 prophylaxis during the main study and the Extension (data cut-off: Jan 2018) were included in this analysis. Mean (SD) age of patients was 34.3 (13.0) years with a median (Q1;Q3) of 7 (2;15) bleeds in the 12 months before enrolment. Most patients (72.1%) had target joint(s) at baseline. Before study, 22 (21.2%) patients were receiving on-demand treatment; the remaining 82 were on regular prophylaxis.
Most patients (n=66, 63.5%) had ≥1 comorbidity of interest. Of those, chronic HCV infection (HCV detection, asymptomatic) was most common (40/66, 60.6%), followed by acute HCV infection (HCV detection, symptomatic, 26/66, 39.4%), HBV infection (20/66, 30.3%), hypertension (17/66, 25.8%), hyperlipidemia (7/66, 10.6%), HIV infection (5/66, 7.6%), and hypertriglyceridemia (2/66, 3.0%). Patients with comorbidities of interest were older (mean age: 41.5 vs 21.9 years, respectively) and had a higher median (Q1;Q3) number of joint bleeds in the previous 12 months (5 [1;12] vs 3 [0;10], respectively) than patients without comorbidities (n=38).
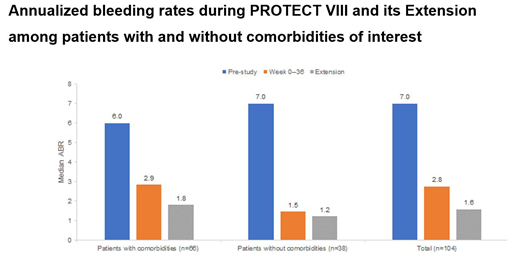
Pre-study, median ABR was 6.0 and 7.0 in patients with and without comorbidities of interest respectively, which decreased to 2.9 and 1.5 respectively during the main study, and further to 1.8 and 1.2 respectively during the Extension (Figure). In all patients with comorbidities of interest, robust improvements in median ABR were observed between the 12-month pre-study period and the main study period, and were maintained or improved in the Extension.
Patients with comorbidities of interest had similar numbers of drug-related adverse events (AEs; 10.6% vs 23.7%), serious AEs (39.4% vs 28.9%) and discontinuations due to AEs (1.5% vs 2.6%) than those without comorbidities of interest during main study and Extension.
Conclusions:
The majority of patients (63.5%) in PROTECT VIII had ≥1 comorbidity of interest. The results from this post hoc analysis indicate that long-term BAY 94-9027 prophylaxis provided excellent control of bleed rates and was well tolerated in patients with severe HA and comorbidities of interest: HIV, HBV or HCV infection or risk factors for CVD.
Miesbach:Biotest: Research Funding, Speakers Bureau; Sanofi: Consultancy, Honoraria; Freeline: Honoraria; Takeda: Consultancy, Honoraria, Research Funding, Speakers Bureau; Novo Nordisk: Consultancy, Honoraria, Research Funding, Speakers Bureau; Grifols: Speakers Bureau; Biomarin: Consultancy, Honoraria; LFB: Consultancy, Honoraria, Research Funding, Speakers Bureau; Sobi: Consultancy, Honoraria, Research Funding, Speakers Bureau; UniQure: Consultancy, Honoraria, Research Funding; CSL: Research Funding, Speakers Bureau; Novartis: Consultancy, Honoraria; Roche: Consultancy, Honoraria; Bayer: Research Funding, Speakers Bureau; Octapharma: Consultancy, Honoraria, Speakers Bureau; Pfizer: Consultancy, Honoraria, Research Funding, Speakers Bureau. Di Minno:Sanofi: Speakers Bureau; Bayer: Consultancy, Honoraria, Speakers Bureau; Kedrion: Speakers Bureau; CSL: Speakers Bureau; Pfizer: Speakers Bureau; Novo Nordisk: Speakers Bureau. Santagostino:Roche: Consultancy, Speakers Bureau; Octapharma: Consultancy, Speakers Bureau; Pfizer: Consultancy, Speakers Bureau; Spark: Speakers Bureau; Kedrion: Consultancy, Speakers Bureau; Bioverativ: Consultancy, Speakers Bureau; UniQure: Consultancy, Speakers Bureau; Sobi: Consultancy, Speakers Bureau; Novo Nordisk: Consultancy, Speakers Bureau; Grifols: Consultancy, Speakers Bureau; Bayer: Consultancy, Speakers Bureau; Shire: Consultancy, Speakers Bureau; CSL: Consultancy, Speakers Bureau; Sanofi: Speakers Bureau. Klamroth:Bayer, Biomarin, CSL Behring, Novo Nordisk, Octapharma, Pfizer, Roche, SOBI, Takeda: Consultancy; Bayer, Novo Nordisk, SOBI: Research Funding. Bayh:Bayer: Employment. Soto:Bayer: Employment. Hermans:LFB: Consultancy, Honoraria, Speakers Bureau; Pfizer: Consultancy, Honoraria, Speakers Bureau; Octapharma: Consultancy, Honoraria, Speakers Bureau; Bayer: Consultancy, Honoraria, Speakers Bureau; Shire: Consultancy, Honoraria, Speakers Bureau; CAF-DCF: Consultancy, Honoraria, Speakers Bureau; Novo Nordisk: Consultancy, Honoraria, Speakers Bureau; CSL: Consultancy, Honoraria, Speakers Bureau; Sobi: Consultancy, Honoraria, Speakers Bureau; Kedrion: Consultancy, Honoraria, Speakers Bureau; Roche: Consultancy, Honoraria, Speakers Bureau.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal