

Background: Hemophilia patients treated prophylactically with emicizumab (Hemlibra®) may experience break-through bleeds or require additional hemostatic coverage for procedures or surgery. Currently available therapies including rFVIIa (Eptacog Alfa (Activated); NovoSeven®) and aPCC (FEIBA®) have been used with Hemlibra to treat bleeding or when additional coverage is required. While NovoSeven appears safe in combination with Hemlibra (HAVEN 1 to 4 clinical trials), thrombotic events have been observed with concurrent use of FEIBA and Hemlibra. While safe and efficacious when used as directed, NovoSeven must be infused intravenously. Ideally, for patients on subcutaneous (SC) prophylaxis with Hemlibra adjunct rFVIIa could be dosed SC too. Marzeptacog alfa (activated) (MarzAA) is a novel rFVIIa differentiated by increased potency and the ability to be administered SC to achieve pharmacologically relevant plasma concentrations. Thus, MarzAA provides a potential solution to address this unmet need in hemophilia therapy.
Objective: Demonstrate the procoagulant potential of MarzAA, NovoSeven or FEIBA alone or in combination with Hemlibra using the thrombin generation assay in platelet poor hemophilia A (HA) plasma. The thrombin generation potential will therefore provide a surrogate marker to assess the potential safety and efficacy of SC MarzAA in combination with Hemlibra.
Methods: A thrombin generation assay was performed using the PPP-Low Tissue Factor and phospholipid containing thrombin generation assay reagent (#TS31.00, Thrombinoscope, Stago). Citrated hemophilia A plasma was spiked with increasing concentrations (0, 25, 50, and 100 µg/mL) of Hemlibra together with various concentrations of each bypassing agent: MarzAA at 0, 0.1, 0.5, 1, 2.5, 5, and 10 µg/mL, NovoSeven at 1, 2.5, 5, 10, and 50 µg/mL or FEIBA at 0.25, and 0.50 IU/ml. Statistical significance was set at α = 0.05.
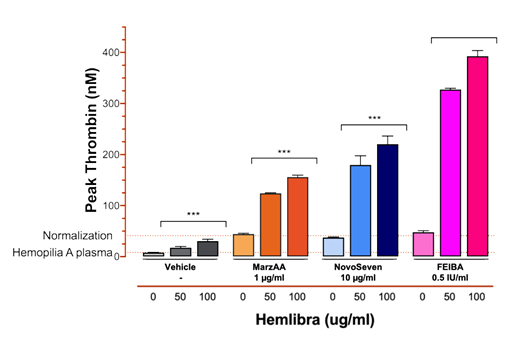
Results: We assessed the relative potencies of MarzAA and NovoSeven in HA plasma. As expected, MarzAA demonstrated an approximate ten-fold increased potency vs NovoSeven. Both rFVIIa compounds increased peak thrombin generation in the HA plasma to the level of normal plasma and beyond. The effect of adding normalizing levels of MarzAA (1 µg/mL), NovoSeven (10 µg/mL) or FEIBA (0.5 IU/mL) to HA plasma containing clinically relevant concentrations of Hemlibra was evaluated (Fig 1). When correcting for the effect of Hemlibra alone, the increase in peak thrombin generation induced by FEIBA was significantly greater than that observed for both MarzAA and NovoSeven (P<0.002). In contrast, the observed increases in thrombin generation for MarzAA and NovoSeven in combination with Hemlibra were statistically indistinguishable. FEIBA was not tested at the highest clinically relevant concentration (2.0 IU/mL) as assay limitations were already approached at 0.5 IU/ml, corresponding to ~25% of the plasma concentration expected for a clinical FEIBA dose of 100 IU/kg. Furthermore, concentrations of MarzAA (5 µg/mL) or NovoSeven (50 µg/mL) 50-fold higher than expected after standard doses were required before peak thrombin generation became statistically indistinguishable from FEIBA at 0.5 IU/mL when all three compounds were evaluated in the presence of Hemlibra.
Conclusion: As assessed by in vitro thrombin generation, equipotent concentrations of MarzAA and NovoSeven exhibit comparable characteristics when spiked into HA plasma containing Hemlibra at clinically relevant concentrations. Based on these data, MarzAA and NovoSeven are expected to behave similarly in combination with Hemlibra when dosed to achieve equipotent plasma concentrations.
Knudsen:Catalyst Biosciences: Employment, Equity Ownership. Kumar:Catalyst Biosciences: Employment, Equity Ownership. Del Greco:Catalyst Biosciences: Consultancy, Equity Ownership. Neuman:Catalyst Biosciences: Employment, Equity Ownership. Levy:Catalyst Biosciences: Employment, Equity Ownership. Blouse:Catalyst Biosciences: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal