

Two recent large case series of patients with HTTP (UK Registry, Blood 2019; 133:1644; International Registry [IR], Haematologica 2019; in press) have reported that stroke is common (UK 25%, IR 31%) and MI is uncommon (IR 4%, UK not reported). The UK case series reported that 5 (7%) patients died; deaths were not reported in the IR case series. No data were reported on the ages when stroke, MI or death occurred (Table 1).
To learn individual patient data, we searched MEDLINE and PubMed and identified 76 case reports/series describing 159 patients. Articles were filtered by publication date from 2001, when HTTP was first defined, through April 2019, and needed to report individual patient data to be included. 5 additional articles that focused on occurrence of stroke were excluded; none focused on MI. HTTP was documented by ADAMTS13 activity <10% and biallelic ADAMTS13 mutations in 152 patients; 7 siblings who had characteristic clinical features of TTP but who had died before the diagnosis of HTTP was documented were also included. Approximately 68 of the 159 patients were included in the IR report; none were included in the UK report. 111 (70%) of the 159 patients were reported because they had novel ADAMTS13 mutations; the 48 other patients were reported for clinical issues (e.g., pregnancy, delayed diagnosis, development of ADAMTS13 inhibitor). Because the objective of these reports was not to describe stroke or MI, we believe that they provide objective evidence for the occurrence and characteristics of stroke and MI.
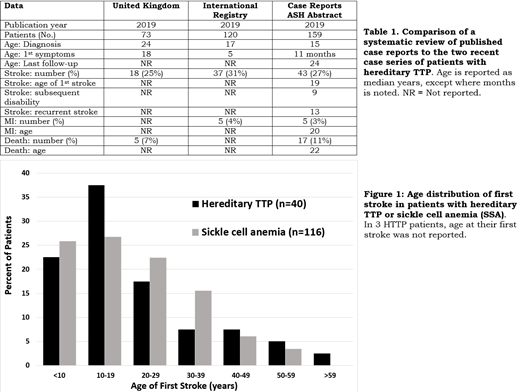
Table 1 describes our 159 patients and compares them to the UK and IR data. 43 (27%) of our 159 patients had a symptomatic stroke, occurring at ages 1 day-79 years (median age, 19 years); two were diagnosed on autopsy. Clinically silent strokes were not reported. 11 of these 43 patients were included in the IR report. 4 of the 43 patients had hemorrhagic strokes; the others were assumed to be ischemic. 4 patients had been receiving regular plasma prophylaxis. 35 (81%) strokes occurred before HTTP was diagnosed. In 2 patients, stroke occurred with neither thrombocytopenia nor anemia. Of the 43 patients with stroke, 13 had recurrent strokes. 9 patients with reported stroke had died at the time of the case report. Of the 34 surviving patients, 9 had residual neurological deficits. 5 (3%) patients had an MI, occurring at ages 2-50 years (median age, 20 years); none were included in the IR report. In 3 patients, MI was diagnosed on autopsy; 4 patients had a prior or concurrent stroke. 17 (11%) patients died at ages 2-79 years (median age, 22 years). The median age of the last follow-up evaluation was 24 years. Among the case reports, not all clinical data described in Table 1 were reported for each patient. The actual frequency of stroke, MI, and death may be greater because we assumed that if these events were not reported, they did not occur.
The frequencies of stroke and MI in our case report data are similar to the frequencies reported by the UK and International Registries, supporting the validity of our data. Our data emphasize the risk for stroke and death at a young age, although follow-up to older ages was limited. Our data also confirm the observation of the IR report that MI is uncommon. The duration of survival of patients with HTTP remains unknown because of the limited duration of follow-up.
Our data for stroke in HTTP patients are strikingly similar to data for stroke in patients with SSA. In both disorders stroke is common and occurs at a young age (Figure 1, SSA data are from Powars, Medicine 2005; 84:363). Among all 1056 SSA patients, 116 (11%) had an overt stroke (median age, 20 years); clinically silent strokes were not reported. Most patients with HTTP (77%) and SSA (75%) had their first stroke before age 30. In the 1056 SSA patients, MI was not reported. The pathogenesis of stroke in patients with HTTP and SSA may be similar: embolic (platelet-von Willebrand factor complexes in HTTP, sickle cell complexes in SSA) rather than atherosclerosis. In both disorders the efficacy of anti-platelet or anticoagulant agents to prevent recurrent stroke is uncertain. The lower frequency of MI in patients with HTTP and SSA suggests that the brain is more vulnerable to the infarction caused by these disorders.
Our data from a collection of case reports must be confirmed by long-term follow-up of individual patients.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal