

Introduction: Over the past decades, there have been substantial improvements in the medical care of sickle cell patients, leading to an increase in life expectancy, despite the fact that the latest studies in adults do not see any change in age at death. Pediatric mortality has declined significantly with the introduction of systematic antibiotics, the preventive care cerebral vasculopathy and therapeutic education for families. It seems important to analyze the morbidity and mortality risks to decide the necessary preventive measures. In this study we will describe the circumstances of death, the profiles of the patients and the risk factors in SCD adult patients.
Materiel and method: We retrospectively reviewed the records of patients which died between 2001 and 2019 and treated in our national referral center (Henri Mondor Hospital) where 3500 patients are followed. Basic biological parameters, chronic and acute complications present in these patients as well as their treatment, median age at death, causes and circumstances of death were identified when the information was available.
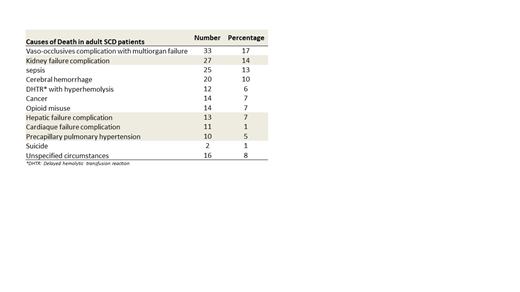
Results: During this period, 198 deaths were recorded or reported by families of patients. 54% were men. Patients ranged in age from 16 to 69 years and median age at death was 37 years IQR [30-47]. Concerning the type of hemoglobinopathy there were 158 homozygous patients (77%), 28 SC (14%), 11 heterozygous Sβ0 (5%) and 4 heterozygous Sβ+(2%).The causes of death are summarized in the Table 1. Patients had chronic terminal stage organ failure in more than 30% of cases, with indication for organ transplantation (renal, hepatic or cardiac) in 60 of them and 10 precapillary PAHs. 18% of patients were dialyzed. The diagnosis of DHTR was not reported in previous studies and probably under-diagnosed but 12 (6%) patients died of hyperhemolysis with multi-organ failure in this study. Nine deaths occurred during pregnancy and 17 during a travel. Biological, echo graphics data and risk factor analysis is ongoing.
Discussion: The median age of death does not seem to improve from the study of Platt et al, however our cohort appears to age, we observed an increase in the number of aged patients over 45. The causes of death have evolved compared to data avaliable from previous studies, chronic organ failures are the leading cause of mortality especially in patients with renal impairment. The prevention of the onset of these complications is one of the new challenges especially renal diseases which was associated with premature mortality. DHTR and brain hemorrhages are new entities probably previously under-diagnosed. Pregnancy remains a risk period, which should strengthen its monitoring.
Michel:Novartis: Consultancy; Rigel: Consultancy; Amgen: Consultancy. Galactéros:Addmedica: Membership on an entity's Board of Directors or advisory committees. Bartolucci:Roche: Membership on an entity's Board of Directors or advisory committees; HEMANEXT: Membership on an entity's Board of Directors or advisory committees; Global Blood Therapeutics: Membership on an entity's Board of Directors or advisory committees; Agios: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; AddMedica: Honoraria, Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal