

Background:
Approximately 57% of individuals with Sickle Cell Disease (SCD) suffer from sleep disorders and poor sleep quality. Poor sleep quality may cause excessive daytime sleepiness and is often associated with psychosocial and clinical factors contributing to disease burden and stress levels. One of these psychosocial factors is John Henryism (JH). Defined as a high-effort, active coping style, JH is used by persons with a strong determination to succeed in the face of chronic stressors. Both sleep and JH have mostly been shown to be negatively associated with cardiovascular health. Living with SCD is a unique stressor and how persons cope with their disease may impact their quality of life and health outcomes. The objective of this study is to 1) evaluate the impact of sleep quality and 2) quantify the effect of sleep quality on high-effort coping among persons with SCD.
Methods:
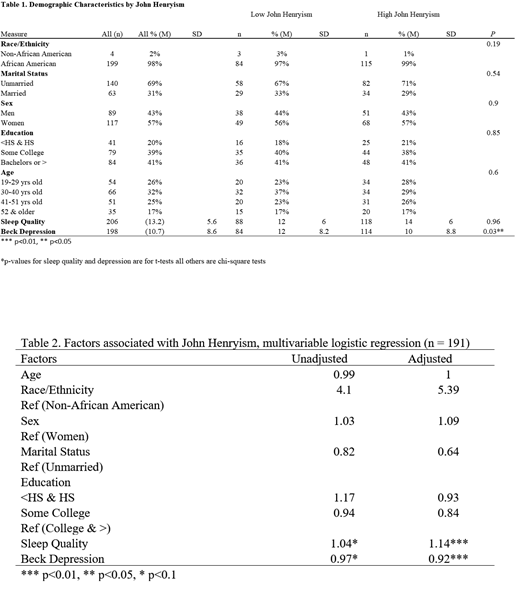
The sample comprised 191 adults aged 19-71 with SCD. Most participants were women (57%) and had a mean age of 39 years (SD+12.2) (see Table 1). All participants were enrolled in the Insights into Microbiome and Environmental Contributions to SCD and Leg Ulcers (INSIGHTS) study (NCT02156102). All participants were administered a variety of psychosocial measures, a comprehensive medical history and physical exam, and provided blood and saliva samples for clinical and research analysis. Our binary outcome assessed participants' high or low utilization of JH coping style by using the John Henryism Active Coping Scale (JHAC12). JHAC12 scores were measured from participant responses to a 12-item Likert scale. Scores range from 12 to 60 with higher scores indicting higher utilization of JH active coping. Based on the median JH score of our participants, scores between 12-50.9 were categorized as low utilization of JH and scores between 51-60 were categorized as high utilization of JH. Predictors included demographic data and psychosocial measures. Sleep quality was assessed via clinical and survey measures. Clinically, obstructive sleep apnea was self-reported during a comprehensive medical exam. The ASCQ-ME sleep survey is a 5-item measure, and was used to ascertain participant sleep patterns within the past seven days. Scores range from 40 to 60. Scores less than 50 are considered abnormal. Multivariable logistic regression was performed to evaluate differences within the cohort.
Results:
Mean ASCQ-ME sleep score of the entire cohort was 46, indicating worse sleep quality for participants compared to the ASCQ-ME national SCD reference cohort. Obstructive sleep-apnea was self-reported by 23 participants (12%). The mean JH score was 52, indicating high utilization of active coping. Poorer sleep quality was associated with higher JH coping (OR:1.14, 95% CI: [1.06-1.22]) (see Table 2). There were no significant associations between utilization of JH active coping with the demographic data including sex, age, education and marital status. Worse sleep quality within the SCD cohort was associated with increased usage of hydroxyurea (r= .16, p<.05), history of cardiovascular disease (r= .13, p<.05), higher pain score at study visit (r=.15, p<.05) and increased systolic blood pressure (r=.18, p<.01).
Conclusion:
Preliminary findings support a relationship between JH and sleep quality in a SCD cohort. In a disease population with high sleep apnea prevalence, these findings have potential clinical implications. Future work should focus on how these psychosocial factors impact sleep and clinical presentation.
Minniti:Doris Duke Foundation: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal