

Background: Sickle cell disease (SCD) is an inherited genetic disorder that results in the formation of sickle hemoglobin (HbS). HbS polymerizes when deoxygenated, deforming erythrocytes and leading to chronic hemolysis, anemia and vaso-occlusion.
Sickle cell nephropathy (SCN) is the term used to describe the renal complications of SCD. Renal vaso-occlusion and hemolysis contribute to the manifestations of SCN which include hyperfiltration and progressive renal impairment. Chronic kidney disease (CKD) is diagnosed if abnormalities in kidney structure or function are present for >3 months. The prevalence of CKD in patients with SCD increases with age, and ~12% of patients progress to end-stage renal disease (Gosmanova et al. J Investig Med 2014; Powars et al. Medicine 2005). There are no treatments approved for CKD caused by SCD. Standard of care (SoC) typically consists of angiotensin-converting enzyme (ACE) inhibitors, angiotensin-receptor blockers (ARBs) and/or hydroxyurea (HU). Evidence for the clinical effectiveness of ARBs and ACE inhibitors has been generated mainly from trials in other causes of kidney disease or short-term studies in SCD.
P-selectin contributes to vaso-occlusion by mediating adhesion of sickled erythrocytes and leukocytes to the endothelium. Crizanlizumab is a humanized monoclonal antibody that binds to P-selectin with high affinity and specificity. In SUSTAIN, crizanlizumab significantly reduced the median annual rate of vaso-occlusive crises compared with placebo (Ataga et al. N Engl J Med 2017). Preclinical data show P-selectin expression in the kidneys and upregulation in response to renal ischemia-reperfusion injury (Singbartl et al. FASEB J 2000; Zizzi et al. J Pediatr Surg 1997). Crizanlizumab may have a beneficial effect in patients with SCD and CKD by blocking P-selectin-mediated multicellular adhesion, reducing the effects of vaso-occlusion in the renal vasculature and slowing the decline in renal function. The aim of the STEADFAST study is to determine if crizanlizumab can slow the progression of CKD due to SCD (EUDRACT no. 2018-003608-38).
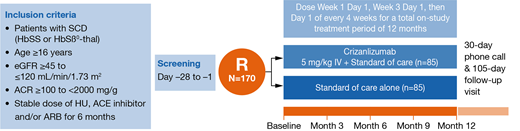
Methods: Approximately 170 patients aged ≥16 years with CKD due to SCD will be enrolled. Eligible patients will have HbSS or HbSβ0-thalassemia genotypes, an estimated glomerular filtration rate (eGFR) ≥45 to ≤120 mL/min/1.73 m2, an albumin-to-creatinine ratio (ACR) ≥100 to <2000 mg/g and be receiving SoC (which includes HU, ACE inhibitors and/or ARBs) for SCD and/or CKD. Patients must have been receiving SoC for ≥6 months and plan to continue at the same dose and schedule until study end. Exclusion criteria include history of stem cell transplant, chronic red blood cell transfusion therapy, acute kidney injury (AKI) within 3 months of study entry, and patients undergoing hemodialysis.
Patients will be randomized to receive crizanlizumab 5.0 mg/kg plus SoC or SoC alone. Patients in the combination arm will receive crizanlizumab 5.0 mg/kg by IV infusion over 30 minutes on day 1 of week 1, followed by a second dose 2 weeks later, after which it will be administered every 4 weeks. The total treatment period is 12 months.
Primary endpoint: proportion of patients with a ≥30% decrease from baseline in ACR at 12 months, based on the intent-to-treat population. A logistic regression model including treatment effects and stratification factors will be utilized and the test (based on the log-odds ratio estimated by the model) will be carried out at the 1-sided significance level of 0.025. Secondary endpoints include mean change in ACR from baseline to 3, 6, 9, and 12 months, proportion of patients with ≥30% decrease in ACR at 6 months, proportion of patients with ≥20% improvement of protein-to-creatinine ratio (PCR) at 12 months, percentage change in eGFR from baseline to 3, 6, 9, and 12 months, and the proportion of patients with progression of CKD (based on decline in eGFR category accompanied by a ≥25% drop in eGFR from baseline) from baseline to 12 months. Exploratory endpoints include improvement in renal and cardiac biomarkers at 3, 6, 9, and 12 months and tricuspid regurgitation velocity (TRV) <2.5 m/s at 12 months among patients with abnormal TRV at baseline.
Conclusion: CKD is a common complication of SCD. The STEADFAST study will evaluate whether crizanlizumab, in combination with SoC, can reduce albuminuria and slow CKD progression, thus providing evidence of a reno-protective effect of crizanlizumab.
Ataga:Novartis: Consultancy, Honoraria, Membership on an entity's Board of Directors or advisory committees; Global Blood Therapeutics: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Emmaus Life Sciences: Honoraria, Membership on an entity's Board of Directors or advisory committees; Bioverativ: Honoraria, Membership on an entity's Board of Directors or advisory committees; Pfizer: Research Funding; Modus Therapeutics: Honoraria. Saraf:Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees; Pfizer: Research Funding. Derebail:RTI: Honoraria; Novartis: Consultancy; Retrophin: Consultancy. Sharpe:Novartis: Consultancy. Inati:Pfizer: Honoraria, Membership on an entity's Board of Directors or advisory committees; Roche: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Honoraria, Membership on an entity's Board of Directors or advisory committees, Research Funding; Novonordisk: Honoraria, Membership on an entity's Board of Directors or advisory committees; AstraZeneca: Research Funding; Global Blood Therapeutics: Research Funding. Lebensburger:Pfizer: Research Funding; Novartis: Consultancy. DeBonnett:Novartis Pharmaceuticals Corporation: Employment. Zhang:Novartis: Employment. Bartolucci:Global Blood Therapeutics: Membership on an entity's Board of Directors or advisory committees; Agios: Membership on an entity's Board of Directors or advisory committees; HEMANEXT: Membership on an entity's Board of Directors or advisory committees; Roche: Membership on an entity's Board of Directors or advisory committees; AddMedica: Honoraria, Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal