

Imagine a scenario in which defective/malignant hematopoietic stem cells (HSCs) are depleted and replaced by healthy HSCs without hematologic or systemic side effects. In this issue of Blood, show that selective CD117+ HSC exchange therapy might become a clinical reality.1
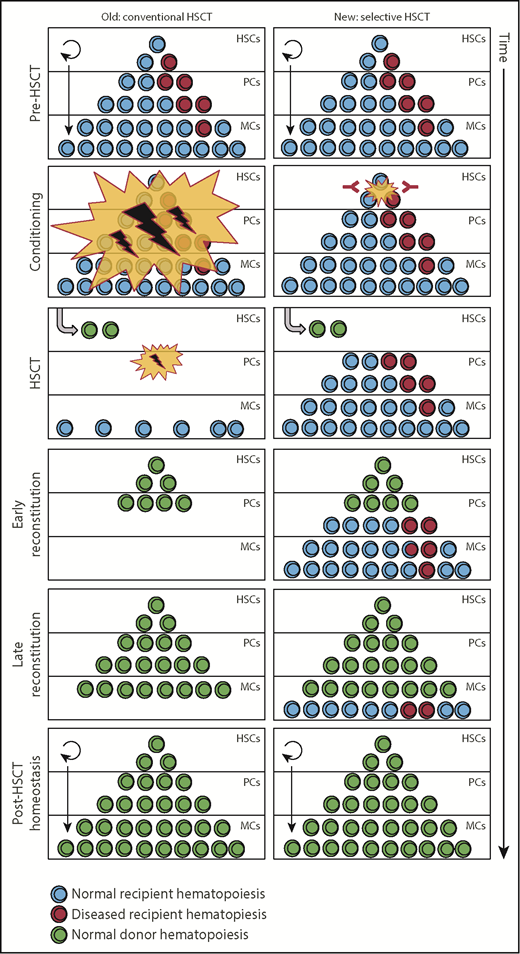
Key differences between conventional (left) and selective immune-mediated (right) conditioning for HSCT. Conventional HSCT conditioning regimens target most hematopoietic cells, including healthy and malignant HS(P)C, and generate nonhematopoietic environmental damage, leading to temporary pancytopenia and nonhematopoietic toxicity. Selective conditioning specifically eliminates HS(P)C (and their diseased counterparts) and subsequent HSCT leads to seamless blood production without nonhematopoietic damage. PCs, progenitor cells; MCs, mature cells.
Key differences between conventional (left) and selective immune-mediated (right) conditioning for HSCT. Conventional HSCT conditioning regimens target most hematopoietic cells, including healthy and malignant HS(P)C, and generate nonhematopoietic environmental damage, leading to temporary pancytopenia and nonhematopoietic toxicity. Selective conditioning specifically eliminates HS(P)C (and their diseased counterparts) and subsequent HSCT leads to seamless blood production without nonhematopoietic damage. PCs, progenitor cells; MCs, mature cells.
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) spearheaded somatic stem cell therapy and cellular immunotherapy. It is now a routine procedure, mostly used with the intention of curing myeloid hematopoietic stem and progenitor cell (HS(P)C)-derived malignancies.2 Success of allo-HSCT depends on 2 elements, that is, on lasting engraftment with physiologic function of the substitute HSCs and cotransferred immune cells as well as on eradication of the underlying host malignant hematopoietic disease. Lasting engraftment of donor HSCs requires creation of bone marrow niche space for HSCs and their descendants as well as suppression of host-versus-graft immune rejection. Eradication of the underlying host disease depends on pre-allo-HSCT therapies, but also critically on the donor immune cell–mediated graft-versus-leukemia (GvL) effect, that is, graft-versus-host disease (GvHD) against the host hematopoietic system, including remaining malignant cells. However, although continuously improving, the overall morbidity of current allo-HSCT remains high, in part caused by pretransplant conditioning (chemotherapy, γ-irradiation, immunological immune depletion) and posttransplant immunosuppression for prevention or treatment of GvHD, and associated infectious complications. This largely restricts allo-HSCT to otherwise fit and healthy individuals, which excludes the majority of patients. Moreover, disease relapse after allo-HSCT remains a major cause of death. Thus, improving selectiveness of preconditioning regimens to efficiently deplete host malignant HS(P)Cs while at the same time creating space for incoming donor HSCs, reducing collateral damage to nonhematopoietic tissue, and preserving as well as augmenting donor immune function against remaining malignant cells, are major challenges in the field.
In this issue of Blood, Pang et al successfully tackle several of these challenges with 1 approach. Using a monoclonal antibody targeting c-Kit (CD117), a transmembrane receptor tyrosine kinase, they demonstrate HSC niche space generation as well as host malignant HS(P)C eradication, followed by sustained engraftment of donor HSCs. Specifically, they show that (1) CD117 is expressed on normal human HSC and myelodysplastic syndrome (MDS) HS(P)C at similar levels; (2) the mouse anti-human CD117 monoclonal antibody SR-1 inhibits binding of the natural ligand stem cell factor (SCF) to CD117; (3) SR-1 inhibits proliferation of healthy human cord blood and bone marrow HS(P)C in vitro and permanently depletes healthy human HS(P)Cs from previously engrafted NSG mice; (4) SR-1 (and AMG 191, a clinical-stage humanized version of SR-1) depletes low-risk MDS from PDX-NSG mice and, upon additional depletion of mouse HS(P)Cs with an anti-mouse CD117 antibody, permits subsequent engraftment of normal human HSCs. They also demonstrate that high-risk MDS, xenografted in NSG mice, was only temporarily reduced by SR-1 treatment alone, and that the reduction was enhanced by subsequent healthy human HSC transplantation. Importantly, in a companion Blood manuscript by the same group, they show that AMG 191 can be safely administered and transiently depletes HS(P)Cs in non-human primates. Furthermore, AMG 191 also can be used in immunodeficient xenografted mice as a human HSC-depleting conditioning regimen that enables transplantation of a second-donor human HSC graft.3
The work on human HSCs and their malignant counterparts by Pang et al builds on prior studies demonstrating HSC “niche-clearing” by a CD117 blocking anti-mouse antibody (ACK2), which permits engraftment of congenic HSCs in immunodeficient recipients.4 This also works in fully immunocompetent mice if Fc-mediated antibody functions are enhanced through blockade of the SIRPα-CD47 myeloid immune checkpoint.5 Alternatively, pretransplant conditioning with ACK2 treatment and low-dose irradiation allows mouse HSC engraftment in immunocompetent mice.6 Excitingly, in parallel findings to the study presented here, it was shown that in immunocompetent mice, a single dose of drug-conjugated anti-mouse CD117 antibody followed by HSCT results in full donor chimerism without impairment of immune functions or mature blood cell counts.7
Taking all this together, it is tempting to speculate about a new area of “selective immune-mediated HSC exchange therapy” in myeloid malignancies as well as in nonmalignant, inherited hematopoietic/immune-system disorders. In this scenario, step 1 would be the exclusive eradication of diseased and healthy host CD117+ HS(P)Cs; step 2 would require termination of the anti-CD117 activity; and step 3 would be transfer of healthy CD117+ HS(P)Cs, which seamlessly produce fully functional hematopoietic cells (see figure). However, several questions still need to be addressed: (1) what is the exact in vivo mode of action of the anti-CD117 targeted therapy and what might be the optimal effector strength of the immune approach in different clinical situations? The current antibodies seem to work both via inhibition of natural ligand (SCF) binding and via Fc-mediated toxicity. One can speculate that anti-CD117 efficacy can be engineered and enhanced by Fc optimization, drug-antibody conjugates (as already done5 ), generation of T-cell engaging and activating antibody constructs, or even by using anti-CD117 chimeric antigen receptor (CAR) T cells with a switch-off mechanism; (2) what will be the on-target toxicities on other hematopoietic and nonhematopoietic cells? CD117 is expressed on HSCs and early myeloid and lymphoid progenitor cells, but also on mast cells, which are relatively abundant in many tissues. CD117 is also expressed in nonhematopoietic tissues as, for example, by certain cells in the central nervous system, interstitial pacemaker cells in the gastrointestinal tract, some kidney cells, and melanocytes. Although no nonhematopoietic toxicities were reported in the in vivo models, there might be species-specific expression and reaction differences. Side effects might depend not only on the variable susceptibility of different cell types toward blockade of SCF signaling but also on the immune-effector strength applied (ranging from nonmodified immunoglobulin G to CAR T cells); (3) can recipient immunosuppression, which is required to prevent incoming HSC rejection and GvHD, both major causes of HSCT-associated morbidity, be relevantly reduced with such an approach in the genetically heterogeneous human population? This may require additional immunological depletion of host cells and possibly transplantation of HSC-enriched grafts with subsequent lymphocyte transfers for protective immunity and GvL.
Although the discussed approaches might still appear visionary, the authors of the study are already testing the clinical translation in patients with severe combined immunodeficiency, which is a situation that resembles the preclinical research (ClinicalTrials.gov identifier: NCT02963064). Indeed, they report encouraging toxicity-free engraftment in the first treated patients.8 Thus, one can be optimistic that studies like the one discussed here will pave the way to “selective HSCT” in hematopoietic malignancy, correction of genetically inherited hematopoietic diseases, and possibly even for the purpose of tolerance induction in solid organ transplantation.9
Conflict-of-interest disclosure: The authors declare no competing financial interests.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal