

Abstract
Introduction: Extracorporeal membrane oxygenation (ECMO) is a form of a cardiopulmonary bypass circuit that is utilized for patients in dire need of cardiac or pulmonary support. The circuit exposes blood to artificial surfaces which leads to platelet activation, clotting and thrombocytopenia. The addition of heparin is required in order to prevent clots from forming along the circuit. Heparin-induced thrombocytopenia (HIT) and heparin induced thrombocytopenia and thrombosis (HITT) are serious adverse effects of heparin treatment characterized by formation of antibodies to heparin platelet factor 4 (PF4) complexed with heparin which leads to thrombocytopenia and a greatly increased risk of arterial and venous thrombosis. The well-established incidence of HIT ranges from 0.5-5% in patients exposed to heparin for more than four days. The reported incidence of HIT in ECMO patients ranges from less than 1% to 8.3%. However this data comes from only a few studies with small sample sizes. Our institution has a large lung center and as a result ECMO is utilized frequently. When patients are suspected to have HIT, they are taken off heparin and switched to a different anticoagulant. For patients without HIT, the switch to a different anticoagulant is unnecessary and exposes the patient to additional risks such as a higher risk of bleeding. Our aim was to calculate the incidence of HIT and HITT at our institution. Furthermore we wanted to examine the platelet trends of all patients on ECMO specifically comparing and contrasting the patients who are deemed true HIT positive vs. all other patients on ECMO.
Methods: We conducted a retrospective analysis of all patients on ECMO at Temple University Hospital from July 1, 2012 to December 31, 2017. The data for this study was drawn from the T'PAU (Temple Population Access Utility) research data warehouse that has successfully merged data from the Epic EMR and the McKesson administrative system that houses important summary data on inpatient admissions going back through July 2012. Our inclusion criteria consisted of all patients on ECMO who had a clinical suspicion of HIT and thus had a screening test sent for HIT, the ELISA polyclonal IgG testing against PF4. The diagnosis of HIT or HITT was confirmed by PF4 antibody positivity with an optical density (OD) >1.0, serotonin release assay (SRA) positivity or a positive PF4 antibody test >0.4 and the presence of thrombosis. Linear mixed-effects model was used to estimate and compare platelet count change over time between true HIT patients and patients who tested negative for the HIT ELISA.
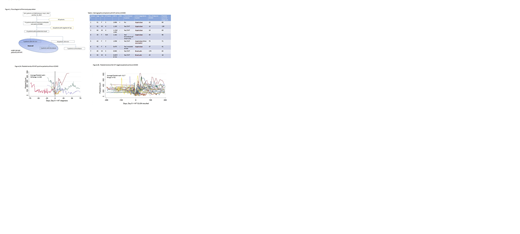
Results: There were 164 patients on ECMO between July 1st, 2012 and December 31, 2017. A total of 77 patients had the HIT ELISA sent while on ECMO. Of those, 15 patients had a positive test result (OD > 0.4) and 62 had a negative test result. Of the patients with positive results, 5 patients had an OD > 1.0. Three of the 10 patients with an OD < 1.0 were found to have thrombosis. Therefore 8 patients had true HIT out of a total of 164 patients on ECMO, for an incidence of 4.88%. There was no difference of the change of platelet count over time between the HIT (n=8) and non-HIT (n=62) groups (P=0.98).
Conclusion: The incidence of HIT in our ECMO patient population is similar to the incidence of HIT in all patients who have been exposed to heparin for four or more days. Patients requiring ECMO are very ill and with the accompanying thrombocytopenia that develops with the initiation of ECMO, the clinical suspicion for HIT is high. Unlike the majority of hospitalized patients, patients on ECMO are a unique population and platelet count trends are not necessarily a clinically reliable indicator for HIT. Our research supports that the full clinical picture should be taken in account when suspecting HIT in patients on ECMO, especially when considering a change in anticoagulation.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal