

Abstract
Introduction: Systemic sclerosis (SSc) is a chronic autoimmune disease with ongoing high disease related mortality. Three randomized controlled trials proofed efficacy of autologous stem cell transplantation (aHSCT) in patients with severe SSc and superiority over the standard cyclophosphamide pulse therapy. Treatment related mortality is a major point of criticism and different treatment regimen are used in different centers.
Methods: This prospective, open, multi-center, non-interventional study of the European Group for Blood and Marrow Transplantation (EBMT) analyzed data for consecutive aHSCT performed in SSc. Every center followed its own local protocol which usually refers to the recent update of the EBMT Guidelines. In order to be eligible for inclusion, patients had to be transplanted for the diagnosis of progressive SSc and aged between 18 and 65 years. Major exclusion criteria were an ejection fraction <40% by cardiac echo, pulmonary arterial hypertension with systolic pulmonary arterial pressure (sPAP) >50mmHg, creatinine clearance <30ml/min, reduced lung function with either FVC <50% or DLCO <30% of predicted values. Concurrent neoplasms, myelodysplasia, severe psychiatric illnesses as well as previously damaged bone marrow had to be ruled out.
Progression free survival (PFS) was chosen as primary endpoint. Response to treatment, defined as the number of patients who achieve >25% improvement of the skin thickness, measured by the modified Rodnan Skin score (mRSS; range 0-51) and/or ≥10% improvement in forced vital capacity (FVC) or hemoglobin-adjusted diffusion lung capacity for carbon monoxide (DLCO) and relapse rate as well as safety considerations were secondary endpoints.
Results: Between 2013 and 2015, 80 patients from 12 centers were followed for a median of 24.1 (5.97 - 59.8) months. Patients had a median age of 43 years at aHSCT and 70% were female. All patients were mobilized with cyclophosphamide (CYC) with a median of 2g/m2 and granulocyte-colony stimulating factor (GCSF) in 98%. In 45% of transplants stem cells were purified using CD34-positive selection. For conditioning, centers used CYC at 200 mg/kg (50 - 240) in 76 patients (95%) or CYC at 100 mg/kg and thiotepa 10 mg/kg in 4 patients. All patients received additional anti-thymocyte globulin (ATG; different brands were used) over 4-5 days.
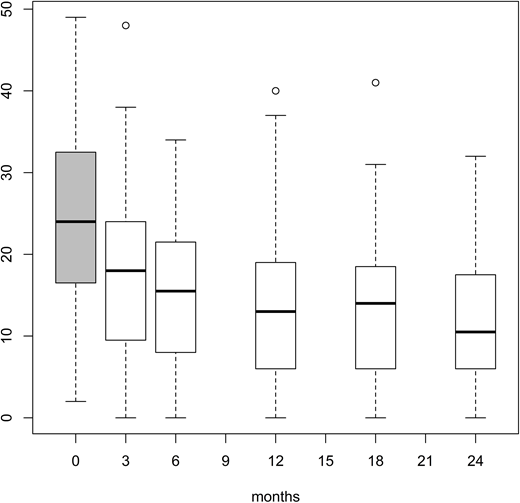
Progression free survival at 1 year was reached by 83.6% of our patients. Response to treatment at 1 year was achieved by 75% (63.7 - 83.2) and 10.1% relapsed or had further progression despite aHSCT. Figure 1 demonstrates the improvement of skin fibrosis over time. Median mRSS decreased from 24 (2 - 49) at baseline to 13 (0 - 40) at month 12, and 10.5 (0 - 32) at month 24. On multivariate analysis, creatine kinase (CK) levels < 250 U/ml, mRSS <24 and lung crepitation at baseline were significantly associated with response to treatment, but especially CD34-positive selection is a strong positive predictor for response to treatment with a hazard ratio of 2.19 as compared to patients treated with non-selected stem-cell.
The 100-day treatment-related mortality for this population was 6.2% (n=5) (CI 2.3 - 13). Three of these 5 patients had a cardiac or cyclophosphamide related event that led to death. During the 24 months of follow up another 3 patients died due to progressive disease, which leads to an overall survival of 91.2% (CI: 85.1 - 97.4) at 2 years.
Discussion: Although aHSCT has been proven effective in SSc, we still do not know which regimen is the best. With data from this non-interventional trial we could demonstrate the effectiveness of aHCST in a daily practice setting. Treatment seems to become safer over time with reduction of TRM from 10% in the European phase III Autologous stem cell transplantation international scleroderma trial (ASTIS; JAMA. 2014; 311(24): 2490-8) to 6.2% in our actual study; mainly due to increasing experience of the centers and exclusion of patients with advanced organ damage. Nevertheless indication for aHSCT should also be driven by negative predictive parameters for disease related mortality and it is fairly unlikely to further reduce TRM in these sick patients.
We also found a potential value of CD34-selection in these patients. As a retrospective approach demonstrated no benefit to the outcome of SSc patient treated with AHSCT (Bone Marrow Transplant.2016; 51(4): 501-5), these findings have to be confirmed by prospective randomized trials.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal