

Abstract
Introduction
Diffuse large B cell lymphoma (DLBCL) is the most common highly aggressive non-Hodgkin lymphoma (NHL) worldwide. The International Prognostic Index (IPI) has been established as a useful prognostic marker, and there have been some proposed markers which could reflect tumor microenvironment including neutrophil, lymphocyte, platelet, serum globulin, ferritin and serum free light chain. C-reactive protein (CRP) is one of the commonly used inflammatory markers, and its clinical relevance has been suggested recently in various malignancies. Serum albumin is a representative marker for nutritional status, and previous studies have presented that hypoalbuminemia might be an indicator of cancer-related inflammation as well. In this point of view, C-reactive-to-albumin ratio (CAR) has been suggested as one of easily-accessible parameters which could be a robust prognostic marker in diverse malignancies such as lung cancer, gastric cancer and colorectal cancer. However, its clinical value has not been assessed in hematologic malignancies. In this study, we evaluated the prognostic effect of CAR in DLBCL.
Methods
This retrospective study included 186 patients who were histologically diagnosed with DLBCL and treated with R-CHOP (Rituximab, Cyclophosphamide, Doxorubicin, Vincristine and Prednisone) between 2006 and 2018 at National Cancer Center, Korea. One hundred forty one cases were identified whose baseline laboratory values including CRP and albumin were available, and then the medical records were reviewed. To define the appropriate cutoff value of CAR in patients with DLBCL, cutoff finder method was applied which had been suggested by Budczies et al., and the most discriminative point was designated by the value of 0.158. Clinical characteristics and outcomes including response rate, overall survival (OS) and progression-free survival (PFS) were investigated between high and low CAR group. Additionally, the clinical value of CAR was compared to the components of IPI for DLBCL as well.
Results
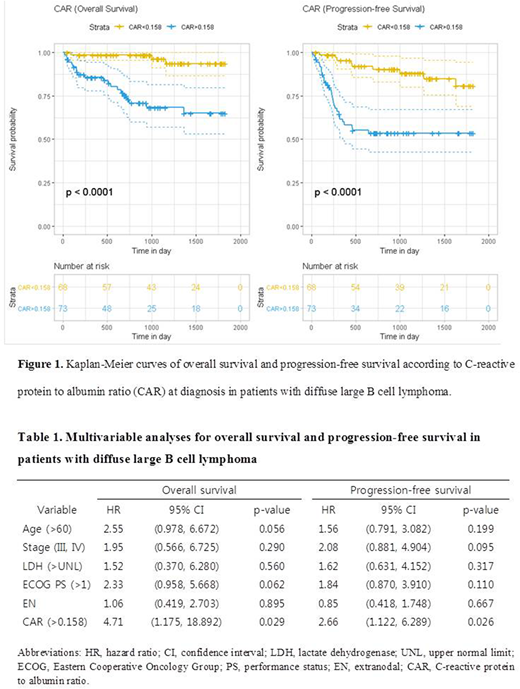
Of all patients, 73 (51.8%) were classified as high CAR group. Male was 42 (57.5%) in high CAR group and 37 (54.4%) in low CAR group. In terms of IPI, 21 (28.8%) were classified into high IPI (score of 4 or 5) in high CAR group - 6 (8.8%) in low CAR group in comparison. Hans criteria was applied to discriminate germinal center B-cell (GCB) subtype to non-GCB subtype by immunohistochemistry and after 12 patients removed due to missing GCB status, 56 (84.8%) in high CAR group was sorted to non-GCB type - 46 (73.0%) in low CAR group to be compared. The high CAR group showed significantly worse complete response (CR) rates to induction R-CHOP therapy (64.4% vs. 92.6%; p<0.001). Median cycles of induction chemotherapy was 6 in all patients and there was no significant difference between both groups (p=0.824). With a median follow-up of 32.5 months, the high CAR group revealed significantly worse 5-year OS (65.0 vs. 93.5%; p<0.0001) and 5-year PFS (53.5 vs. 80.7%; p<0.0001) (Figure 1). In univariable Cox analysis, high CAR was a statistically significant prognostic factor for both 5-year OS (HR 8.04, 95% CI 2.384-27.139; p=0.001) and 5-year PFS (HR 4.44, 95% CI 2.109-9.341; p<0.001). Along with CAR, all components of IPI was statistically significant for both OS and PFS, except age at diagnosis (HR 1.95, 95% CI 0.908-4.207, p=0.087) for 5-year OS. In multivariable analyses with adjustment for age (>60), stage (III, IV), lactate dehydrogenase (LDH) (>upper normal limit), Eastern Cooperative Oncology Group (ECOG) performance status (>1) and the number of extranodal involvement (>1), high CAR showed statistically significant results for both 5-year OS (HR 4.71, 95% CI 1.175-18.892; p=0.029) and 5-year PFS (HR 2.66, 95% CI 1.122-6.289; p=0.026) (Table 1).
Conclusions
In conclusion, CAR might play an additional role to IPI in prognostication of patients with DLBCL considering the fact that it is simple, objective and easy to obtain.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal