

Abstract
Introduction: Mainstay of chemotherapy in acute myeloid leukemia (AML) is induction with a goal to achieve morphological complete remission (CR) as evident by less than 5% blasts. Post remission strategies then focus on either consolidation chemotherapy or allogeneic bone marrow transplantation (aBMT). However, not all patients by this remission criterion achieve long term remission and a subset of patients' relapse. This relapse originates from further expansion chemoresistant clones. Detection of minimal residual disease (MRD) following chemotherapy, early in the course of treatment, is highly predictive of outcome and offers a window of opportunity to intensify treatment and prevent relapse as seen in ALL. Here, we describe assessment of immunophenotypic MRD using a 10-colour two tube assay and a combination of difference from normal and leukemia associated immunophenotype (LAIP) approach in patients of adult AML.
Methods: We accrued 310 patients of adult (>18 years) AML, other than with t(15;17), over a 66-month period (1st July 2012- 31st December 2017) after obtaining informed consent. All patients received standard induction chemotherapy. MRD testing was done post induction and after first consolidation with high dose cytarabine. Patients accrued from 1st July 2012 to 28th February 2015 (85 patients) were processed using a three tube 8 colour MRD assay. Subsequently samples of 225 patients were processed using a two tube 10 colour MRD assay. Identical panel was used for diagnostic sample, post induction and post consolidation. 500,000 events were acquired per tube with the 3-tube assay and 1.6 million events per tube obtained per tube with the 2 tube, 10 colour assay. Analysis of MRD was done using Kaluza 1.3 by a combination of difference from normal approach that focused on the development of Myeloid progenitors to mature cells and LAIP approaches. Cytogenetic studies by conventional karyotyping and FISH was done as per NCCN version 2 2014 recommendations. Patients were classified into favorable, intermediate and poor cytogenetic risk. The presence of FLT3-ITD, NPM1 and CEBPA mutations were detected by a fragment length analysis-based assay. Overall survival (OS) was calculated from date of diagnosis to time of last follow up or death. Relapse free survival (RFS) was calculated from date of CR till time to relapse or death or last follow up if in CR. Results of the MRD assays, cytogenetic and molecular risk groups were analyzed for their impact on OS and RFS using log rank test.
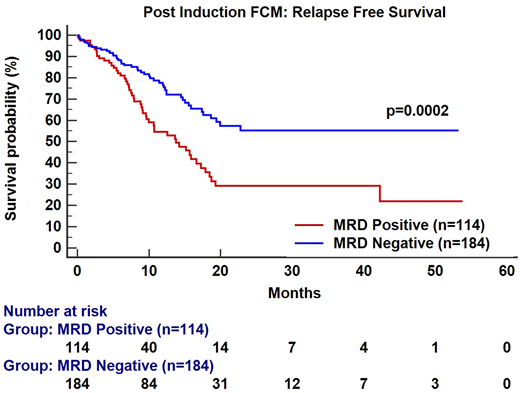
Results: The median age of entire cohort was 33 years (M : F = 1.6 : 1). Based on cytogenetics, 35.1% were classified as favorable risk whereas 52.5% and 12.2% were intermediate and poor risk respectively. FLT3-ITD, NPM1 and CEBPA mutations were detected in 21.9%, 29.0% and 7.7% of patients respectively. Post induction MRD was assessed in 298 patients of which 114 (38.3%) had detectable residual disease (range 0.004-22.6%, median:0.9%). Post consolidation MRD was assessed in 186 patients of which 49 (26.4%) were MRD positive (range 0.002-19.8%, median: 0.37%).The 3 year OS, RFS and median RFS of the entire cohort was 59.0%, 44.8% and 18.7 months respectively. Poor risk cytogenetics as expected was predictive of inferior OS (median OS = 14.6 months vs not reached, p=0.05) as well as RFS (median RFS = 9.3 months vs 18.6 months, p=0.003 respectively). FLT3, NPM1 and CEBPA mutations were not informative as predictors of outcome.The presence of MRD at post induction time point predicted an inferior OS [(p=0.08), HR:1.53; 95% CI (0.93-2.51)] & RFS [(p=0.0002), HR:2.14; 95% CI (1.4-3.3)] as compared to the MRD negative group. Similarly, patients harboring MRD at the end of consolidation had an inferior OS [(p=0.04), HR:1.83; 95% CI (0.94-3.6)] & RFS [(p=0.02), HR:1.79; 95% CI (1.04-3.09)] as compared to the MRD negative group. On multivariate analysis post induction FCM MRD emerged as the most important independent prognostic factor predictive of inferior outcome for RFS [(p=0.01); HR:2.14; 95% CI (1.17 - 3.4)] followed by poor cytogenetic risk [(p=0.05); HR:1.8; 95% CI (1.0 to 3.26)].
Conclusion: Our data demonstrates that MRD by flow cytometry at end of induction as well as consolidation are important prognostic factors together with known factors such as high risk cytogenetics. AML MRD is a very useful guide for post remission strategies in AML and should be incorporated into routine treatment algorithms.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal