

Abstract
Cooperative group oncology trials have led to dramatic improvements in outcomes for children with cancer, but the current method of reporting adverse events (AEs) is inefficient and potentially ineffective. Like all cooperative oncology groups, AEs on Children's Oncology Group (COG) clinical trials are reported by clinical research associates via case report forms using the National Cancer Institute Common Terminology Criteria system. Despite the extensive resources needed for AE reporting, there is evidence that AEs may not be accurately reported. However, there are no data on the sensitivity, specificity and positive and negative predictive values (PPV, NPV) of AE reporting on pediatric or adult cooperative group oncology trials. This study sought to determine these operating characteristics for AE reporting for COG clinical trial AAML0531, the most recently completed clinical trial for de novo acute myeloid leukemia (AML) in children.
Chart abstraction was performed by a single pediatric oncologist on patients enrolled on COG clinical trial AAML0531 at 5 hospitals in the United States. Presence or absence of the following 12 grade III or higher AEs was determined for each hospital day: hypertension, hypotension, hypoxia, adult respiratory distress syndrome (ARDS), anorexia, typhlitis, disseminated intravascular coagulation (DIC), microbiologically proven viridans group streptococcal bacteremia (VGS), microbiologically proven invasive fungal infection (IFI), pain, seizure, and acute renal failure. The definitions for the gold standard of chart abstraction were defined a priori. Using the daily AE assessments based on chart review, the presence or absence of each toxicity was determined for each chemotherapy course. These data were then merged with COG adverse event data that includes grade III or higher toxicities for each patient by chemotherapy course. The percentages of chemotherapy courses with each toxicity were determined for chart abstraction and COG data. Sensitivity, specificity, PPV and NPV for COG AE reporting of the 12 toxicities were determined by comparing to the gold standard of chart abstraction data. Age, gender, race and ethnicity were determined from COG data.
COG clinical trial AAML0531 enrolled 1028 patients between August 14, 2006 and June 15, 2010. Chart abstraction was performed on 99 of these patients (373 courses). Compared to all patients enrolled on AAML0531, the 99 patients were younger (mean age 8.0 vs. 9.3 years, p = 0.04), and a larger percentage was African American (18.2% vs. 11.5%, p = 0.05). No differences were observed in gender (female: 48.5% vs. 50.4%, p = 0.72) or ethnicity (Hispanic: 18.2% vs. 18.4%, p = 0.96). In the COG AE report, the rates of toxicities ranged from 0.3% of courses (seizure) to 18.8% of courses (anorexia). In the chart abstraction data the rates of toxicities ranged from 0% of courses (seizure) to 37.0% of courses (pain). Table 1 shows the sensitivity, specificity, PPV and NPV for the 12 targeted toxicities. For toxicities with 10 or more identified events, the sensitivity of COG data ranged from 18.2% (DIC) to 70.0% (hypotension). Of significant concern, sensitivity was less than or equal to 50% for eight toxicities, including hypertension (38.5%), hypoxia (25.3%), anorexia (49.6%), VGS (49.2%), and pain (21.7%). The PPV ranged from 50% (IFI and ARDS) to 100% (DIC and renal failure).
Sensitivity, Specificity, PPV, NPV of 12 Targeted Toxicities
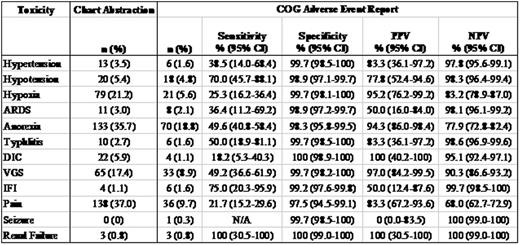
In this cohort of 99 patients treated on COG clinical trial AAML0531, the sensitivity of COG adverse event reporting was relatively low for all but one AE and was less than or equal to 50% for eight of the 12 targeted toxicities. Although PPV was high for most toxicities, it was not 100% for many, indicating that false positive results occur for nearly all of the evaluated AEs. This data demonstrates that the current system of AE reporting on cooperative group oncology trials has modest sensitivity and a demonstrable false positive rate. Work is ongoing to further refine these estimates and to develop improved AE reporting methodologies.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal