

Abstract
Allogeneic hematopoietic cell transplantation (HCT) is a potentially curative treatment option for patients with acute myeloid leukemia (AML). The impact of lymphocyte recovery on post- transplant outcomes has been suggested but has not been evaluated in a homogeneous population of AML patients. The present study attempted to evaluate the impact of lymphocyte recovery at 28 days post-HCT in a homogeneous population of 212 patients with AML that underwent HCT between 1999 and 2011 at the Princess Margaret Hospital, Toronto, Canada. All patients in the study group received peripheral blood stem cells as a graft source. Patients were divided into two groups: those with absolute lymphocyte count (ALC) ≥0.5x109/L (n=122, 57%) and those with ALC <0.5x109/L (n=90, 43%), at day 28 post-transplant.
Median age of all patients was 49 years (range 18-70), 102 patients (48%) were female. HCT was performed in first complete remission (CR1) for 134 patients (63%) and second complete remission (CR2) for 78 patients (37%). Cytogenetics at diagnosis were available in 189 patients (89%). Donors were matched related (n=145, 68%) or matched unrelated (n=67, 32%). Myeloablative conditioning was administered to 131 (62%) patients, 81 (38%) received reduced-intensity conditioning (RIC) regimens. Median follow up duration among survivors was 49 months (range 7-120 months).
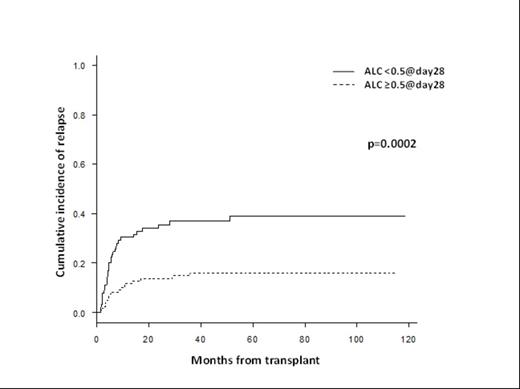
Univariate analysis demonstrated overall survival (OS) was significantly different in favor of the group with ALC ≥0.5x109/L vs those with ALC <0.5x109/L (p=0.016) with a 3-year OS of 57% vs 39% respectively. The cumulative incidence of relapse (CIR) was significantly lower in the group with ALC ≥0.5x109/L vs those with the ALC <0.5x109/L (p=0.0002), with a 3-year CIR of 16% vs 37% respectively (Figure). Cumulative incidences of non-relapse mortality (NRM) were not significantly different between the two groups (p=0.22).
Multivariable analysis for OS and NRM did not demonstrate ALC ≥0.5x109/L at 28 days post-transplant to be an independent prognostic factor. Multivariable analysis for CIR demonstrated that ALC ≥0.5x109/L at 28 days post-transplant is an independent prognostic factor decreasing the risk of relapse compared to ALC <0.5x109/L (p=0.015, HR=0.47, 95%CI=0.25-0.86), which implies that early lymphocyte recovery suggests lower risk of relapse post-transplant. Significant decrease in CIR was also seen with the occurrence of chronic graft-versus-host disease (GvHD) (p=0.00002, HR=0.29, 95%CI=0.16-0.51), while increased CIR was associated with the use of RIC regimens (p=0.03, HR=1.9, 95%CI=1.1-3.5).
The present study concludes that lymphocyte recovery with ALC ≥0.5x109/L at day 28 post transplant is associated with decreasing risk of relapse in a homogeneous population of AML patients that underwent allogeneic peripheral blood HCT, but without overall survival benefit.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal