

Abstract
HLA haploidentical relatives could be useful alternative donor option for patients without HLA matched family donor who need relatively urgent stem cell transplantation. However, steroid refractory GVHD and virus infections were critical issues in this setting due to HLA mismatched barrier. Donor derived cellular therapies could be suitable options to improve the outcome of this strategy.
Twenty three children (9 male, 14 female) underwent HLA haploidentical stem cell transplantation in Nagoya University hospital from 2004 to 2013. The median age was 8 years [range 1 – 15years] with 7 AML, 6 ALL, 5 aplastic anemia, 2 JMML, 1 CMML, 1 CAEBV and 1 LCH. All the patients received both bone marrow combined with G-CSF mobilized peripheral blood stem cells to increase the number of infused donor stem cells. Total 15mg /kg of rabbit antithymocyte globulin (ATG) were given as in vivo T cell depletion in preconditioning regimen. Taclolimus and short term MTX were used for GVHD prophylaxis. CMV and EBV specific cytotoxic T cells were tried to expand from donor peripheral blood mononuclear cells if the patient and the donor shared either HLA A2402 or A0201/A0206 as treatment options for drug resistant virus infections since 2008. Mesenchymal stem cells were also expanded from donor bone marrow for the option of treatment for steroid refractory GVHD since 2009. All the donors were one of parents of patient’s except for one brother. HLA disparity between patient and donor at HLA A, B, and DR loci were three loci in 12 patients and two loci were in other 11 patients.
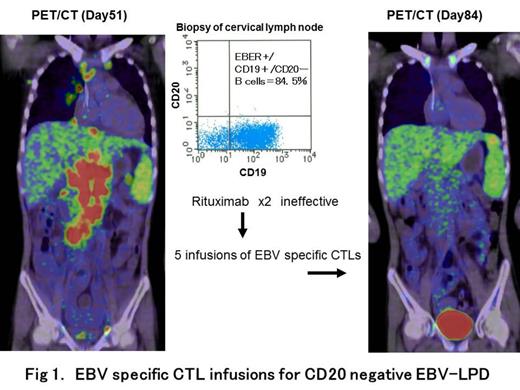
All the patients achieved engraftment with median 18 days [range 14 – 29 days]. Acute GVHD grade II or more were seen in nine patients. Six of them developed steroid refractory GVHD and received Infliximab. Four of them received Daclizumab as well. Among them, two patients developed uncontrolled grade IV GVHD (One patient developed diarrhea more than three litters with blood and another patient developed Grade IV liver GVHD) even after combination therapy of Infliximab and Daclizumab. Two infusions of donor bone marrow derived MSC were given in these two patients and GVHD were diminished. CMV reactivations were seen in 16 and 3 of them developed both GCV and Foscanet resistant CMV infection and donor derived CMV specific CTL infusions were effective to eradicate CMV-DNA in their blood without inducing GVHD. EBV reactivations were seen in 12 and empiric rituximab infusion was effective in 11. One patient developed CD20 negative EBV associated lymphoproliferative disorder and 5 course of donor derived EBV specific T cell infusions eradicate EBV-DNA in his blood and PET positive lymphadenopathy was diminished. BK virus cystitis were seen in four. Cause of death were 8 leukemia relapses, one adenovirus fluminant hepatitis on day 123, one CMV ventriculitis on day 378 and one sepsis on day 509.
Donor virus specific CTLs and mesenchymal stem cells were useful options for HLA haploidentical stem cell transplantation to reduce early transplantation related mortality.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal