

Abstract
Abstract 988
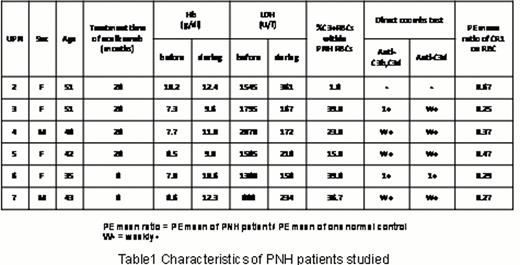
Paroxysmal nocturnal hemoglobinuria (PNH) is a hematologic disorder characterized by the clonal expansion of hematopoietic stem cells that are incapable of glycosylphosphatidylinositol (GPI)-anchor biosynthesis, due to an acquired somatic mutation in the PIGA gene. Affected progeny cells are deficient in all GPI-anchored surface proteins, including the complement regulators CD55 and CD59. Deficiency of CD55 and CD59 accounts for the intravascular hemolysis. Eculizumab is a humanized monoclonal antibody against complement component 5 (C5), thereby inhibiting terminal complement-mediated hemolysis. Eculizumab treatment has significantly reduced hemolysis and transfusion dependency, and improved anemia. However, the hematologic benefit varies considerably among patients. Lactate dehydrogenase levels remain slightly elevated and haptoglobin levels remain low in some patients suggesting residual low level hemolysis. Remarkable extravascular hemolysis mediated by C3 opsonization of PNH red blood cells (RBCs) in some patients with PNH receiving eculizumab has been reported (Blood 113,4094,2009). Complement receptor type 1 (CR1) has a crucial role in dissociation of C3/C5 convertases which activate C3. To explain the mechanism of extravascular hemolysis mediated by C3 opsonization in patients with PNH receiving eculizumab, the kinetics of CR1 and C3 in six patients with PNH (UPN2 to 7) who are treated with eculizumab at Osaka University Hospital were analyzed (Table1).
We first confirmed that patients with PNH (UPN2 to 5) being treated with eculizumab had C3 positive RBCs with variable degree (1.8%-39.8%) and C3 positive RBCs were solely identified within CD59 negative RBCs, whereas healthy controls had only CD59 positive/C3 negative RBCs and untreated patients had both CD59 positive and negative/C3 negative but no C3 positive RBCs. Certain number of C3 positive RBCs were identified from immediately after the first initiation dose of eculizumab, and the proportion of C3 positive RBCs continuously increased with 14 weeks time course in two patients (UPN6 and 7) who could be monitored from before treatment. Then, the proportion of C3 positive RBCs was monitored at the interval of 15 months during treatment, and the proportion of C3 positive RBCs increased in all patients (Figure 1). At this moment, no one had significant clinical symptoms of extravascular hemolysis, and only UPN3 and 4 showed weak positivity in conventional direct anti-globulin test (DAT) at some points. However, DAT using monospecific anti-C3b plus anti-C3d antibody or anti-C3d antibody alone became positive in five out of six cases except for UPN2.
Since CR1 has a crucial role in dissociation of C3/C5 convertases, especially under the conditions of CD55 deficiency, such as PNH, we analyzed the expression levels of CR1 on RBCs. The expression levels of CR1 on RBCs negatively well correlated with the percentage of C3 positive RBCs (Correlation=-0.979) (Figure 2). Since allelic variant of CR1 was known, we screened six patients and no homozygous variant known to express low levels of CR1 was identified. Only heterozygous variant was identified in UPN5 who express slightly low levels of CR1 compared to control (0.47). Then, the kinetics of CR1 and C3 during RBC maturation were analyzed in fractions of reticulocytes and mature RBCs. The proportion of C3 positive RBCs tended to increase, whereas the expression of CR1 tended to decrease during RBC maturation in four patients (UPN3,4,5 and 7).
Thus, we confirmed that patients with PNH started to have C3 positive RBCs mediated by the treatment of eculizumab without exception, and the proportion of C3 positive RBCs increased during treatment. Most patients showed positive DAT using monospecific anti-C3b/anti-C3d antibody, even if there is no significant clinical symptoms of extravascular hemolysis. We also identified that the patients expressing high levels of CR1 tended to have low proportion of C3 positive RBCs, and the expression of CR1 tended to decrease with increasing the proportion of C3 positive RBCs during RBC maturation. We have successfully established several methods to monitor the kinetics of CR1 and C3, although current data are still not conclusive because analyzed patients had little symptoms. Therefore, we have conducted the research project to recruit the patients having significant clinical symptoms of extravascular hemolysis.


No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal