

Abstract
Abstract 3808
Approximately 10–15% of patients with myelodysplastic syndromes (MDS) have a hypocellular bone marrow (BM) at diagnosis. Some studies have suggested hypocellular MDS may have an adverse prognostic impact, but this is controversial. In the Phase 3 randomized AZA-001 study, AZA prolonged overall survival (OS) in patients with higher-risk MDS compared with conventional care regimens (CCR) (Lancet Oncol, 2009). However, the efficacy and tolerability of AZA in the subset of patients with hypocellular MDS has not been determined.
This post hoc analysis was conducted to determine whether the prolongation of OS observed with AZA compared with CCR in the AZA-001 study is influenced by baseline BM cellularity. We also sought to explore the tolerability of AZA treatment in patients with higher-risk MDS and hypocellular BM.
Study design of AZA-001 is reported elsewhere (Lancet Oncol, 2009). Briefly, patients with higher-risk MDS (FAB: RAEB, RAEB-t, or CMML, and IPSS Int-2 or High risk disease) were randomized to AZA (75 mg/m2/d SC × 7d q 28d) or to CCR (supportive care, low-dose Ara-C [LDAC], or intensive chemotherapy [IC]). In the current analysis, patients were divided into 2 groups based on centrally reviewed baseline BM biopsy samples which confirmed the diagnosis of MDS (J. Bennett): a hypocellular (≤30%) group and a non-hypocellular (>30%) group. OS was assessed using Kaplan-Meier methods and treatments were compared by log-rank analysis.
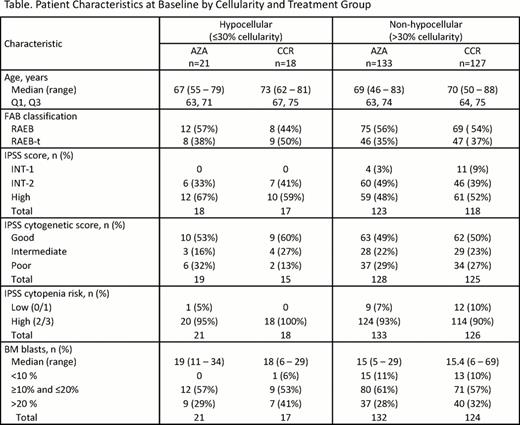
Of 358 patients in AZA-001 (AZA n=179, CCR n=179), BM cellularity data were available for 299 patients (AZA n=154, CCR n=145). At baseline, 87% of patients (n=260) had non-hypocellular BM and 13% of patients (n=39) had hypocellular BM. Of patients with hypocellular BM in the CCR group (n=18), 7 patients (39%) received supportive care, 9 (50%) LDAC, and 2 (11%) IC. In general, baseline characteristics were similar between the hypocellular and non-hypocellular BM groups. Similarly, age, % BM blasts, cytogenetics, cytopenias, and transfusion dependence, were generally balanced across treatments within the 2 cellularity groups (Table). Median (range) duration of AZA treatment cycles in hypocellular patients was 35.5 (28–54) days and in non-hypocellular patients was 33.0 (15–75) days. Response (complete or partial response [CR+PR]) rates in hypocellular patients treated with AZA were 0% and with CCR were 5.6% (p=0.4615); and hematologic improvement (HI) rates were 52% and 41%, respectively (p=0.532). In non-hypocellular patients treated with AZA or CCR, rates of CR+PR were 7.5% and 0.8%, respectively (p=0.010); and HI rates were 48% and 28% (p=0.001), respectively. The improvement in OS in AZA-treated patients was more pronounced in the hypocellular group than the non-hypocellular group, whereas OS in CCR-treated patients was similar regardless of BM cellularity (Figure). Median OS was significantly prolonged with AZA vs. CCR in both the hypocellular and non-hypocellular groups. In patients with hypocellular BM, at 33 months median OS was not reached (NR; 95% CI: 19.2, NR) in the AZA arm vs. 16.9 months (95% CI: 11.1, 19.3) in the CCR arm (p=0.001). In patients with non-hypocellular BM, median OS in the AZA arm was 21.1 months (95% CI: 16.2, 34.7) vs. 15.3 months (95% CI: 9.3, 17.6) in the CCR arm (p=0.012). Safety and tolerability in the two BM cellularity groups were similar to that seen in the overall AZA-001 study (Lancet Oncol, 2009). Frequencies of grade 3–4 hematologic AEs in AZA-treated patients in the hypocellular and non-hypocellular groups were similar: anemia (9.5% vs 14.7%, respectively), febrile neutropenia (9.5% vs 11.6%), leukopenia (14.3% vs 13.2%), neutropenia (61.9% vs 60.5%), and thrombocytopenia (61.9% vs 58.1%).
In this post hoc analysis, the prevalence of patients with hypocellular MDS was 13%, consistent with the reported prevalence in the general MDS population (Bennett, 2009). The survival advantage with AZA vs. CCR in both baseline BM cellularity groups observed in this analysis was consistent with the overall OS advantage with AZA shown in AZA-001. These findings suggest AZA is a safe and effective treatment option for patients with BM hypocellularity.
Patient Characteristics at Beseline by Cellulerity and Treatment Group

Seymour:Celgene Corporation: Consultancy, Honoraria, Speakers Bureau, Travel support Other. Bennett:Celgene Corporation: Consultancy. List:Celgene Corporation: Consultancy. Mufti:Celgene Corporation: Consultancy, Research Funding, Speakers Bureau. Gore:Celgene Corporation: Consultancy, Research Funding. Fenaux:Celgene: Honoraria, Research Funding. Hetzer:Celgene Corporation: Employment, Equity Ownership. Songer:Celgene Corporation: Employment, Equity Ownership. Skikne:Celgene: Employment, Equity Ownership. Beach:Celgene Corporation: Employment, Equity Ownership.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal