

Abstract
Abstract 272
The treatment of Thrombotic Thrombocytopenic Purpura (TTP) with therapeutic plasma exchange (TPE) with Fresh Frozen Plasma (FFP) and/or Cryopoor Plasma (CPP) replacement is well established. This process adds plasma ADAMTS-13 activity and removes plasma ADAMTS-13 inhibitor. Limited data has indicated combination of 5% albumin in the first half of the procedure followed by FFP in the second half of the procedure is effective in treating TTP. Theoretical calculation of addition of exogenous ADAMTS-13 is still substantial because ADAMTS-13 infused initially is removed as the plasma exchange procedure progresses. A 50% reduction of FFP would decrease the number of donor exposures and transfusion reactions associated with human plasma. Further, plasma of limited supply, such as AB plasma, can be more effectively used.
We report a retrospective comparison of TPE for TTP using all FFP versus 5% Albumin/FFP (AFFP) replacement fluid. One health system with two closely connected tertiary campuses with common Hematology/Oncology services and Transfusion Medicine services treated 17 idiopathic TTP patients (March/2009 – June/2012) with documented very low ADAMTS-13 levels (<10) and high inhibitor levels (≥0.4). All other thrombotic microangiopathies were excluded from this comparison. One campus treated 10 patients with FFP and the other campus treated 7 patients with AFFP. Daily one plasma volume TPE was performed until target platelet count was achieved and the patient was then tapered off TPE. For AFFP replacement, 50% of the replacement fluid was 5% albumin given in the first half of the procedure followed by FFP for the second half. Additional medical therapy was managed by the same Hematology/Oncology service.
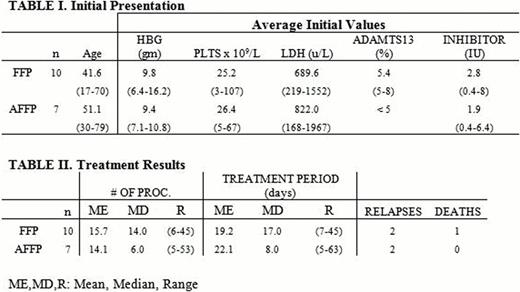
Table 1 shows that the FFP versus the AFFP groups at presentations are comparable. Table 2 indicated FFP versus AFFP treatment is comparable. For the FFP and AFFP groups respectively, mean number of total procedures: 16 vs. 14, length of time from first TPE to last TPE 19 vs. 22 days, Relapses 2 vs. 2, and deaths 1 vs. 0.
The use of AFFP as replacement fluid for idiopathic TTP does not appear to be inferior to 100% FFP replacement. Length of treatment, rate of recovery, and relapse rate are comparable. There were more deaths in the FFP cohort but the low number of observations limits the significance. AFFP fluid replacement should be considered for TPE in idiopathic TTP.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal