

Abstract
Abstract 4295
Although cytarabine plus anthracycline (7+3 or 7+5) regimens are commonly used for induction therapy in patients (pts) with acute myeloid leukemia (AML) and there have been improvements in the treatment of AML in younger adults, there is no standard of care in pts with relapsed or refractory (R/R) AML. Treatment options for older pts and those with R/R disease remain limited.
Clofarabine (JC0707) is a purine nucleoside analog approved in the United States (US) and European Union for the treatment of pediatric pts with R/R acute lymphocytic leukemia (ALL). In a phase II study from the US, single-agent clofarabine showed activity and acceptable toxicity in pts ≥ 60 years with untreated AML and adverse prognostic factors (Kantarjian, J Clin Oncol 2010;28:549–55). The purpose of this phase I open-label, multi-center study is to assess the safety, tolerability, and pharmacokinetics of clofarabine monotherapy in elderly Japanese pts with newly diagnosed AML for whom standard induction chemotherapy is unlikely to be of benefit or Japanese adult pts with R/R AML.
Adult pts (20–74 years) with R/R AML according to World Health Organization (WHO) criteria and elderly pts (60–74 years) with newly diagnosed AML were eligible to participate. Additional inclusion criteria included Eastern Cooperative Oncology Group (ECOG) performance status of 0 to 2 and no prior hematopoietic stem cell transplant.
The study utilized a standard 3 + 3 dose escalation method; 3 pts enrolled in each dosing cohort, 3 additional pts were added to cohorts where dose-limiting toxicities (DLTs) were observed. The maximum tolerated dose (MTD) was defined as the dose level below that for which 2 DLTs were observed. Based on prior clinical trials in the US, pts were to be treated with clofarabine 20 mg/m2/day (IV over 1 hr), 30 mg/m2/day, or 40 mg/m2/day for one 5 day cycle in cohorts 1, 2 and 3, respectively. Pts with evidence of hematologic response after one cycle could receive up to a maximum of 3 cycles. The primary endpoints of this study were MTD, safety, and pharmacokinetic (PK) parameters.
Until June 2011, 14 pts were enrolled and treated in this trial: cohort 1 (n=3), cohort 2 (n=6), and cohort 3 (n=5). Bioanalytical determination of clofarabine concentrations in plasma samples showed an increased concentration with increased dosage. No DLTs were noted in cohort 1 (20 mg/m2). Among the first 3 pts in cohort 2 (30 mg/m2), only 1 patient experienced DLT (reversible, grade 4 elevated ALT). Additionally, 2 pts in cohort 3 (40 mg/m2) experienced DLTs (grade 3 elevated ALT [n=1]; grade 3 elevated amylase [n=1]). Thus, the MTD was determined to be 30 mg/m2.
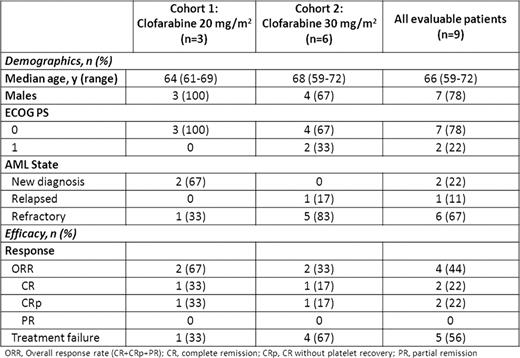
Preliminary safety and efficacy data are available for 9 of these pts and presented herein. Overall, the most common all cause, non-hematologic toxicities were nausea and headache (89% each), rash and elevated ALT and AST (78% each), malaise (56%), pneumonia and hypokalemia (44% each), and elevated bilirubin and vomiting (33% each). Grade 3 or 4 toxicities were primarily hematologic and infectious occurring in 89% and 67% of patients, respectively. Only one patient developed a treatment-related serious adverse event (SAE) (herpes zoster). There were no AE related deaths and no patients discontinued therapy as a result of an AE. Two patients achieved complete remission (CR) and 2 patients achieved CR without platelet recovery (CRp), for an overall response rate (ORR) of 44% (Table 1).
Preliminary Demographic and Efficacy Data
Additionally, plasma samples were obtained from all patients for PK evaluation; plasma concentration data from all 14 patients will be presented.
Clofarabine monotherapy was well tolerated at doses up to 30mg/m2 and showed preliminary evidence of activity with 44% ORR in elderly newly diagnosed AML or adult Japanese pts with R/R AML, warranting further investigations.
Off Label Use: Clofarabine (JC0707) is an investigational agent in Japan; this abstract assesses its use in adult AML patients. Ewesuedo:Sanofi Oncology: Employment. Tabata:Genzyme (a Sanofi company): Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal