

Abstract
Abstract 2870
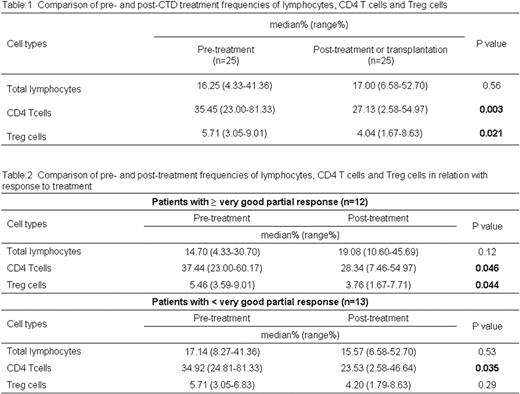
Regulatory T (Treg) cells are one of the master regulators in maintaining tolerance and immune homeostasis. Several studies in hematological and non-hematological malignancies revealed that increased level of Treg cells significantly impede the anti-tumor responses. Moreover, in non-hematological malignancies Treg cells correlate inversely with patient's survival (Beyer et al, 2006, Blood). Here in this study we evaluated the prognostic significance of Treg cells in multiple myeloma (MM) patients and influence of chemotherapies on Treg cells. Patients and Method: In this study a cohort of 74 newly diagnosed MM patients were recruited and all patients gave informed consent. Median age of the patient cohort was 67 years (range: 38–88). According to international staging system (ISS) patients were characterized as ISS1=20(27%), ISS2=27(36%), ISS3=25(34%) and undetermined=2(3%). Patients were treated with following treatment regimens: low or high dose combination of cyclophosphamide, thalidomide plus dexamethasone (CTD- 54/74), bortezomib, doxorubicin plus dexamethasone (5/74), and cyclophosphamide, doxorubicin plus dexamethasone (4/74). Eleven patients did not receive any treatment. Using multiparameter flowcytometry all the MM subjects peripheral blood (PB) samples were analyzed for total lymphocytes, CD4 T cells and Treg cells. For comparison, 10 healthy volunteers PB samples were also assessed. Results: Phenotypically, CD4 T cells were assessed based on the expression of CD4 marker and Treg cells were characterized as CD4+CD25hi+FoxP3+. The frequencies of total lymphocytes were significantly reduced in MM than healthy volunteers [median% (range %)= 16.88(2.77–45.93) vs. 36.96(29.42–53.69); P<0.0001]. CD4 T cell numbers were similar between MM patients and healthy volunteers [median% (range %)= 38.17(15.02–81.33) vs. 40.03(30.58–52.16); P=0.34]. Contrasting to lymphocyte and CD4 T cell counts, Treg cells were significantly increased in MM patients compared to healthy volunteers [median% (range %)= 5.22 (2.57–11.73) vs. 3.00 (1.96–3.59); P<0.0001]. Twenty five patients were followed and their PB samples were assessed after CTD treatment (15/25) or transplantation (10/25). Post-treatment or transplantation assessment showed significant reduction in the frequencies of CD4 T cells and Treg cells compared to pre-treatment, whereas lymphocyte numbers were similar (Table: 1). With regard to treatment responses, ≥ very good partial response (VGPR) was achieved in 12 patients (complete response-3/12 plus VGPR-9/12) and 13 patients achieved < VGPR (partial response-7/13, minimal response-1/13 and progressive disease-5/13). Patients with ≥ VGPR showed significant reduction in the frequencies of CD4 T cells and Treg cells after treatment compared to pre-treatment. However, patients with < VGPR showed only significant reduction for CD4 T cells (Table: 2). No significant association was observed between pre- and post-treatment frequencies of Treg cells with treatment responses. Time to progression (TTP) data was available for 44 patients. The median follow-up period of this patient cohort was 11 months (range: 4–18). We separated the patients into two cohorts, such as patients (23/44) with higher Treg cell count (≥ 5%) and patients (21/44) with lower Treg cell count (< 5%). Univariate analysis showed inferior TTP for patients with higher Treg cell count compared to patients with lower Treg cell count (13 months vs. median not reached; P=0.013). Other clinical variables did not hold significance for TTP in this cohort. As well, Cox regression multivariate model ensured inferior TTP for cohort with higher Treg cell count compared to cohort with lower Treg cell count (P=0.045). Conclusions: It is well known that myeloma patients suffer from various immune abnormalities and Treg cells also mediate immune dysfunctions. Unprecedentedly, our data suggest that progression in subgroup of myeloma patients was due to higher infiltration of Treg cells in the peripheral blood. This data also encourages that Treg cells could be a potential target in myeloma patients along with tumor cells. As well our finding showed that CTD efficiently depleted the Treg cells in patients who achieved ≥ VGPR. This study was supported by respective grants MSM0021622434, LC06027, IGA NS10406, IGA NS10408, and GACR P304/10/1395.
Off Label Use: cyclophosphamide, thalidomide and dexamethasone.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal