

Abstract
Abstract 2040
Consolidative high dose chemotherapy [HDT] and autologous peripheral blood hematopoietic stem cell transplant [auto-HSCT] is an effective treatment modality for multiple myeloma [MM]. Many advances during the last two decades have lead to significantly improved progression free survival [PFS] and overall survival [OS]. Novel agents [thalidomide, lenalidomide and bortezomib] have replaced conventional chemotherapy during induction due to superior response rates. Randomized trials have defined melphalan as the optimal preparative regimen prior to auto-HSCT. Further recent attempts to improve the preparative regimen have included the addition of oral busulfan or bortezomib to melphalan. We performed a single institution, retrospective analysis in order to compare the outcomes of patients with newly diagnosed MM, treated with either conventional chemotherapy or novel agents, who received melphalan versus BEAM [carmustine, etoposide, cytarabine, melphalan] regimens during their first auto-HSCT.
179 MM patients were treated or referred to the University of Nebraska Medical Center for auto-HSCT between 1999 and 2010. All patients in the analysis were treated with induction regimens that included either VAD [vincristine, doxorubicin, dexamethasone], thalidomide, lenalidomide, or bortezomib. We compared PFS and OS in patients receiving melphalan [140 or 200 mg/m2 (N=103)] versus BEAM [carmustine 300 mg/m2, etoposide 100 mg/m2, cytarabine 100 mg/m2, and melphalan 140 mg/m2 (N=76)]. Characteristics of patients were compared using univariate statistics. The probabilities of PFS and OS were estimated using the Kaplan-Meier method, while the Cox proportional hazard regression analysis was used to evaluate the association between conditioning regimen and PFS or OS while adjusting for significant covariates.
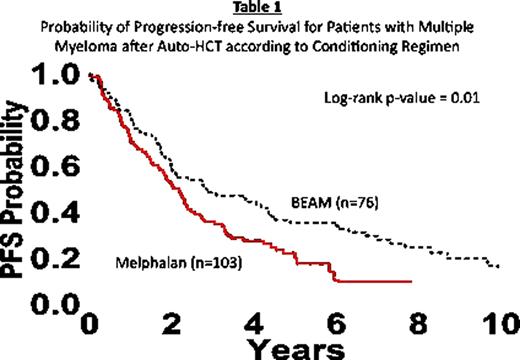
No statistical significant differences in age, sex, race, median time from diagnosis to transplant, and disease stage at diagnosis were seen between the two groups. Disease stage at transplant differed between melphalan {CR (complete response) = 5, PR (partial response) = 89, other = 9} versus BEAM {CR = 22, PR = 51, other = 3} [p<0.001]. Median duration of follow-up of survivors for melphalan {60 months} was less than BEAM {100 months} [p<0.0001]. PFS {70 vs 82 at one year [p=0.08], 20 vs 36 at 5 years [p=0.01] – Table 1} and OS {89 vs 88 at one year [p=0.83], 46 vs 59 at 5 years [p=0.05] – Table 2} were improved with BEAM. When compared to melphalan, BEAM was associated with a 30% reduction [HR 0.70, p=0.07] in disease progression and a 37% reduction in treatment failure [HR 0.63, p=0.01]. In addition, BEAM was associated with a 31% reduction [HR 0.69, p=0.009] in death compared to melphalan. With regard to disease progression, treatment failure and death in patients treated with BEAM, patients less than or equal to 60 years old experienced an advantage over patients greater than 60 years old, as demonstrated by increased reductions in disease progression [68% reduction, p=0.005], treatment failure [53% reduction, p=0.005], and death [76% reduction, p=0.006].

The use of BEAM as a regimen for newly diagnosed MM patients during their first auto-HSCT was associated with improved PFS and OS when compared to melphalan. BEAM was associated with a reduced risk of disease progression, treatment failure and death. No significant differences were observed based on treatment-related toxicity or treatment related mortality. The improved PFS and OS were independent of the remaining confounding variables in the multivariate analyses with the exception of CR prior to first auto-HSCT and followup time. Therefore, these are potential contributors to the differences in PFS and OS. Further analyses stratified by cytogenetics, induction therapy, therapy after progression of first auto-HSCT and maintenance therapy are required to further characterize the PFS and OS advantage, as well as to potentially identify a specific patient population that may benefit more from BEAM than melphalan. Nevertheless, BEAM appears to be an efficacious, well tolerated preparatory regimen to be considered in future prospective clinical trials.
Vose:GSK: Research Funding; Millenium: Research Funding; Celgene: Research Funding; BMS: Research Funding; Exelixis: Research Funding; SBio: Research Funding; Pharmacyclics: Research Funding; Genentech: Research Funding.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal