

Abstract
Abstract 1684
The early assessment of molecular responses to tyrosine kinase inhibitors (TKI) used as a front line therapy for chronic phase chronic myeloid leukemia (CML) might represent an attractive surrogate marker for survival and help to discriminate poor prognosis patients (pts). So, we studied in a retrospective bicentric institutional analysis a series of 142 de novo CP CML pts diagnosed between 2000 and 2011, receiving imatinib (IM) 400 mg daily (n=85 pts), second generation TKI (TKI2) (n=57 pts) with 37 dasatinib (DAS) pts 100 mg daily and 20 nilotinib (NIL) pts 600–800 mg daily as front-line therapy, enrolled or not in clinical trials. All pts were assessed for their cytogenetic and molecular responses (local RQ-PCR for BCR-ABL, expressed as BCR-ABL/ABL ratios (IS) in %). Failure to TKI was defined as progression to accelerated phase or blast crisis, death, loss of complete hematologic response, loss of complete cytogenetic response, confirmed loss of major molecular response (MMR), discontinuation of TKI because unacceptable toxicity, primary cytogenetic resistance. The definition of progression included the same variables except the two last. Pts were considered in MMR with a BCR-ABL/ABL ratio ≤0.1% (IS). There were 87 males (61%) and 55 females with a median age of 55 years (21–83) at diagnosis. Six pts (4%) had an additional clonal abnormality, 4 a masked Philadelphia (Ph) chromosome, and 4 a variant Ph. Three pts had an atypical BCR-ABL transcript, all in IM400 group. Sokal scores were low for 37 (26%), intermediate for 61 (43%) and high for 43 (31%) (1 NA), and Euro scores were low for 49 (35%), intermediate for 78 (55%), and low for 14 (10%) (1 NA). These scores were similarly balanced in the IM400, NIL and DAS groups. The median time between diagnosis and TKI was 1 (0.9–1.28) month, not significantly different between TKI groups. The median follow-ups were 56, 37, and 19 months for IM400, NIL and DAS groups respectively. Fifteen percent, 6%, and 14% of pts achieved MMR at 3 months (M3) (p=ns); 31%, 37%, and 40% at M6 (p=ns); 55%, 70% and 71% at M12 (p=ns); 67%, 90% and 87% at M18 (p=ns) in IM400, NIL and DAS groups respectively, taken into account the limited numbers of pts at latest time-points in the 2 TKI2 arms. Twenty-three pts achieved 4-log molecular response MR4 in IM400, 10% in NIL and 11% in DAS at latest follow-ups. Four pts died, 3 in blast crisis in IM400 group and 1 for unrelated reason to disease or treatment in NIL group. A multivariate analysis adjusted on progression-free survival (PFS) performed, did not identify any significant parameter including age, gender, Sokal and Hasford scores, ACA, type of transcript, interval between diagnosis and TKI start. The progression-free survival (PFS) was 94 (83–100)% for pts achieving M3 MMR vs 86 (74–100)% if MMR occurred at later time points vs 86 (73–100)% for pts that never achieved MMR (p=0.02). There was no difference for PFS between the 3 TKI (log-rank p=0.9). None of the M3 MMR switched to another treatment, whereas 10 % of other pts did so for resistance (n= 10, 1 and 2 for IM400, NIL and DAS respectively), 9% for intolerance (n=10, 1 and 4), and 3% for other reasons (n=4, 0 and 0) with no difference between the 3 drugs (p=0.74). The failure-free survival (FFS) was 95% for M3 MMR pts vs 65% for pts with MMR occurring at later time points, versus 0% if MMR has not been achieved (p<0.0001). Again, there was no difference in the FFS survival rates at any times between the 3 TKI (p=0.78), (figures 1a & 1b below).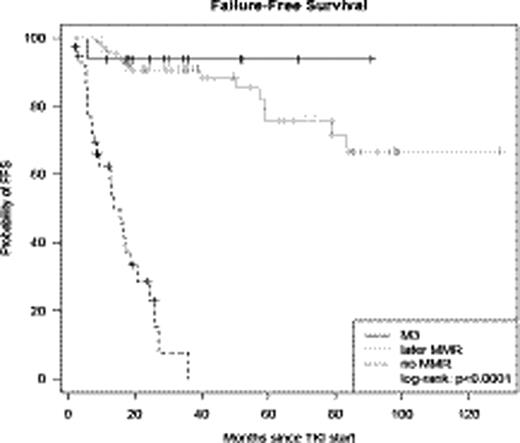
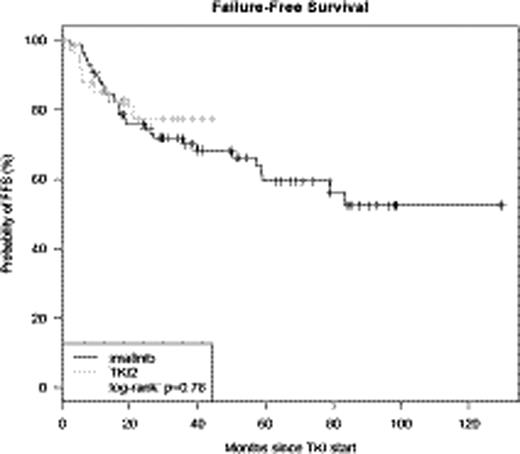
Fig 1a:

FFS M3 MMR vs later MMR vs no MMR
Fig 1b:

FFS IM400 vs TKI2
In conclusion, this academic retrospective study suggests that the achievement of M3 MMR represents a major prognostic factor for progression-free and failure-free survival in CP CML pts on TKI.
Disclosures:
Nicolini:consultant for Novartis Pharma France and Bristol Myers Squibb: Consultancy. Michallet:consultant for Novartis Pharma France and Bristol Myers Squibb: Consultancy. Mahon:consultant for Novartis Pharma France and Bristol Myers Squibb: Consultancy. Etienne:consultant for Novartis Pharma France and Bristol Myers Squibb: Consultancy.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal