

Abstract
Abstract 1217
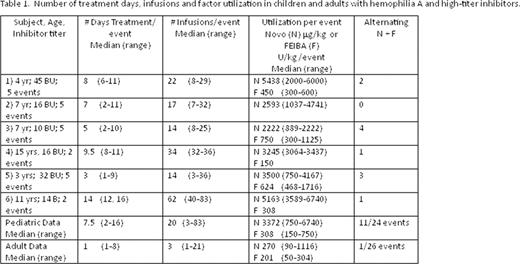
Children with hemophilia A and high-titer inhibitors suffer frequent severe bleeding events and often respond to bypassing agents more poorly than adults resulting in increased dosing and cost. Aims: This study was conducted to determine the amount and variability of bypass agent therapy currently given to children with inhibitors at a large combined adult and pediatric hemophilia treatment center in comparison to treatment of adult inhibitor patients. Methods: All subjects were enrolled onto a single institution prospective inceptional cohort study of bleeding disorders with appropriate IRB-approved consent and assent. All children who developed high-titer inhibitors were treated with immune tolerance induction, and children treated with bypassing agents primarily represent difficult inhibitors. Data regarding treatment agents, dose and duration were extracted for 24 bleeding events in 6 children in comparison to comparable data on 26 bleeding events in 5 adults with high-titer inhibitors. Treatment decisions were made clinically by academic hematologists in consultation with hemophilia nurses, patients and parents based on perceived severity of bleeding events and therapeutic response. Treatment was given as recombinant factor VIIa (NovoSeven, N, n=28), prothrombin complex concentrates (FEIBA, F, n=10) or alternating doses of both (A, n=12). Median results for individual children and aggregated adult data are shown on Table 1. Children received seven times the treatment doses and duration compared with adults. In addition, children received both N and F for half of the bleeding events, while this was used for only one adult event. Treatment duration in children was not affected by initial dose or dose frequency of N (p > 0.05 for both). Bleeding events were severe and difficult to manage; significant long-term morbidity in these 6 children include ankle arthropathy in 3, elbow contracture following compartment syndrome in 2 and quadrucep pseudotumor in 1.
Children with hemophilia A and inhibitors experience bleeding episodes that are poorly responsive to both N and F, resulting in higher dosing, longer duration and enormous costs. Children require better inhibitor therapies. Clinical trials of new bypassing agents designed specifically for children are urgently needed.
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal