

Abstract
Abstract 1014
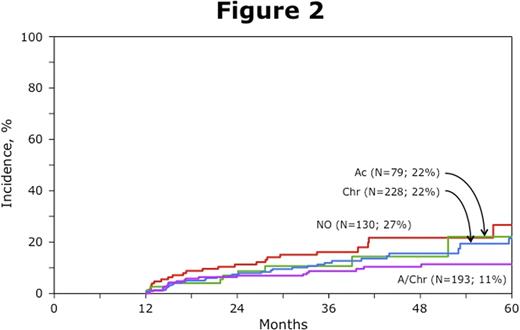
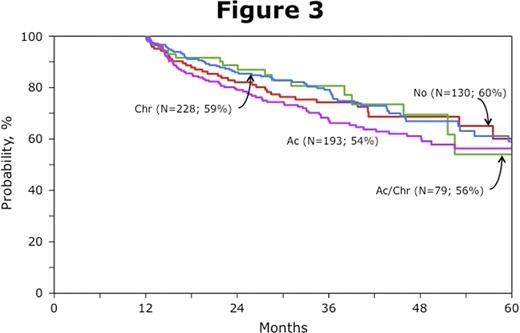
GVHD can induce non-relapse transplant-related mortality (TRM) and can augment the GVL effect after hematopoietic cell transplantation (HCT). The net impact on survival represents a balance of these parallel immunologic influences. We examined the effect of acute and/or chronic GVHD on risks of late (beyond 1 year) relapse, TRM and disease-free survival (DFS) after allogeneic HCT for acute myeloid leukemia (AML) and myelodysplastic syndrome (MDS); and probed any differential influences using either myeloablative (MA) or reduced intensity conditioning (RIC). Landmark analysis was performed at 1-year as all acute GVHD and over 95% of chronic GVHD had occurred within 1 year after HCT. Eligible patients had to be disease-free and alive at 1-year. Between 1997–2006, 5741 patients with AML/MDS received HCT; of these, 2369 patients survive disease-free at 1-year. Approximately 70% had AML and 30% MDS. Disease status at HCT for the study cohort (alive disease-free at 1-year), were 40% in first complete remission (CR), 17% in 2nd or later CR and 43% in relapse. MA conditioning recipients (70% of the cohort) had a median age of 42 years; RIC (30% of the cohort) median 56 years. For analysis we compared: 1) patients without acute or chronic GVHD [baseline control group; No], 2) acute GVHD only [Ac], 3) chronic GVHD only [Chr] and 4) both acute and chronic GVHD [Ac/Chr]. Following MA conditioning late relapse risks were not significantly different in the 4 groups: No GVHD (RR 1.0), Ac GVHD only (RR 0.96, p=0.87), Chr GVHD only (RR 1.01, p=0.94) and Ac/Chr GVHD (RR 0.96, p=0.81) (Figure 1). In contrast, TRM risks were higher with any GVHD; Ac GVHD only (RR 2.31, p=0.004), Chr GVHD only (RR 3.43, p<0.0001) and Ac/Chr GVHD (RR 4.50, p<0.0001). Consequently, after MA HCT, treatment failure (TRM or relapse) was similar with Ac GVHD only (RR 1.32, p=0.13) compared to those with No GVHD, but was significantly higher with either Chr GVHD only (RR 1.62, p=0.0002) or Ac/Chr GVHD (RR 1.85, p<0.0001). Following RIC regimens, relapse risks were similar with no GVHD (RR 1.0), Ac GVHD only (RR 0.70, p=0.37) and Chr GVHD only (RR 0.72, p=0.22), but relapse was significantly lower in patients Ac/Chr GVHD (RR 0.49, p=0.02) (Figure 2). TRM was similar with No GVHD, Ac GVHD only (RR 1.25, p=0.63) and Chr GVHD only (RR 1.36, p=0.36), but TRM was higher in patients with Ac/Chr GVHD (RR 2.69, p=0.002). Consequently, treatment failure was similar in all groups: No GVHD (RR 1.0), Ac GVHD only (RR 0.88, p=0.67), Chr GVHD only (RR 0.93, p=0.73) and Ac/Chr GVHD (RR 1.22, p=0.32) (Figure 3). These data suggest that when using MA conditioning either Ac and/or Chr GVHD has an adverse effect on TRM without compensatory augmentation of GVHD-associated GVL, thus leading to worse DFS. MA HCT must use better strategies to prevent any GVHD. However, using RIC regimens, Ac plus Chr GVHD limits risks of relapse, but without adverse effect on survival and disease-free survival. Therefore, following RIC HCT, GVHD-associated GVL may be more important in limiting late leukemia recurrence. Overly suppressive approaches to eliminate any GVHD might increase relapse risks after RIC HCT for AML and MDS.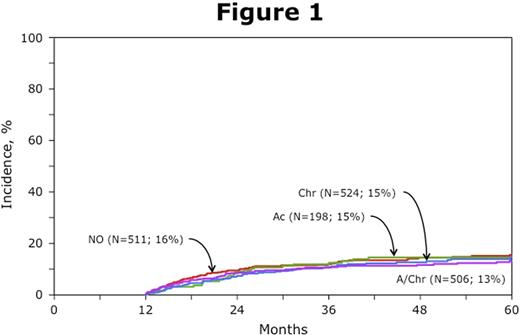



Disclosures:
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal