

Abstract
Abstract 661
CB hematopoietic stem cell transplantation (CBT) can be successful even if donor and recipient are not fully matched for human leukocyte antigens (HLA). This may result, at least in part, from tolerance-inducing events during pregnancy, but this concept has not been tested to date. Hence we analyzed the impact of fetal exposure to NIMA of the HLA-A, -B antigens or -DRB1 alleles on the outcome of 1121 pts with hematologic malignancies. All pts received single CB units provided by the NYBC, for treatment of ALL (N=451), AML (N=376), CML (N=116), MDS (N=79), other (N=99); 22% were transplanted in advanced stage. Median age was 9.7 years (range: 0.1-67); 29% of recipients were >16 years. Most pts (96%) received myeloablative cytoreduction. Sixty-two pts received fully matched grafts while 1059 received units mismatched (MM) for one or two HLA antigens. Of these, 79 (7%) had a MM antigen which was identical to a donor NIMA (Example: Pt: A1, A3; CBU: A1, A2; mother-CBU: A1, A3; A3 is NIMA). NIMA match was found in 25 recipients with one HLA MM and 54 of those with two MM. The NIMA match was identified after the transplant and was not used in unit selection. In multivariate analyses, NIMA matched transplants (NMTs), showed faster neutrophil recovery (RR=1.3, p=0.043), even for grafts with cell dose <3×107 (RR=1.6, p=0.053). There was no difference in the incidence of acute (grade II-IV) or chronic GvHD. 3-year relapse risk (cumulative incidence 22%) was reduced compared to 1 or 2 HLA MM no NIMA matched transplants, especially in pts with myelogenous malignancies given units with 1 HLA MM (RR=0.2, p=0.074). Further, 3-year transplant-related mortality was reduced (RR=0.7, p=0.034), particularly in pts ≥5 years old (RR=0.5, p=0.006), as was the 3-year overall mortality (RR= 0.7, p=0.029 and RR=0.6, p=0.015, respectively). As a result, in the NMTs, treatment failure (relapse or death) was significantly lower, particularly in pts ≥5 years (RR=0.7, p=0.019) and DFS was significantly improved (figure) and was similar to that of the 0 HLA MM group. These findings are the first indication that donor exposure to NIMA can improve post-transplant survival in unrelated CBT and might reduce relapse. We propose to include the NIMA of CB units in search algorithms. Thus, for pts lacking fully HLA matched grafts, HLA MM but NIMA matched CB units could be selected preferentially, since no adverse effects were seen. This strategy of selecting HLA MM grafts with optimal outcome effectively “expands” the current CB Inventory several-fold.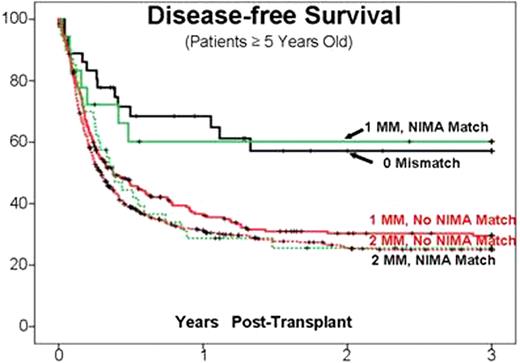

| Patient Group | N | RR | (95% Cl) | p value |
|---|---|---|---|---|
| 0 MM | 36 | 0.5 | (0.3–0.8) | 0.005 |
| 1 MM / NIMA Match | 18 | 0.4 | (0.2–0.9) | 0.026 |
| 2 MM / NIMA Match | 40 | 0.8 | (0.5–1.2) | 0.309 |
| 1 MM / No NIMA Match | 229 | reference group | ||
| 2 MM / No NIMA Match | 487 | 1.1 | (0.9–1.3) | 0.365 |
| Patient Group | N | RR | (95% Cl) | p value |
|---|---|---|---|---|
| 0 MM | 36 | 0.5 | (0.3–0.8) | 0.005 |
| 1 MM / NIMA Match | 18 | 0.4 | (0.2–0.9) | 0.026 |
| 2 MM / NIMA Match | 40 | 0.8 | (0.5–1.2) | 0.309 |
| 1 MM / No NIMA Match | 229 | reference group | ||
| 2 MM / No NIMA Match | 487 | 1.1 | (0.9–1.3) | 0.365 |
Disclosures:
No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal