

Abstract
Abstract 358
During the induction of normal immune responses, activated B cells secrete the chemokines CCL3 and CCL4 for recruitment of regulatory T cells (Nat Immunol. 2:1126-32, 2001). This may represent a mechanism enabling cognate interactions between rare antigen-specific T and B cells. We previously reported that CCL3 and CCL4 RNA and protein are induced in CLL cells by co-culture with nurselike cells and after B cell antigen receptor (BCR) cross-linking (Blood 113:3050-8, 2009). We found higher levels of CCL3 and CCL4 in ZAP-70 positive cases, and CCL3 and CCL4 secretion was abrogated by the Syk inhibitor R406. These findings suggest that CCL3/CCL4 secretion by CLL cells correlates with the signaling capacity of the BCR. Also, we previously noticed higher plasma levels of CCL3 and CCL4 in CLL patients, when compared to healthy controls.
In this study, we measured CCL3 and CCL4 plasma levels by ELISA in 351 CLL patients, and correlated CCL3 and CCL4 levels with various prognostic markers, including RAI stage, immunoglobulin heavy chain variable region gene (IgVH) mutational status, ZAP-70, β2 microglobulin, CD38, white blood count (WBC), and cytogenetic subgroups. We found that the concentrations of CCL3 and CCL4 were significantly higher in plasma samples from CLL patients who had CLL cells that used unmutated IgVH genes or that expressed ZAP-70 or CD38, or who had an advanced stage of their disease (see Table 1). For example, the mean CCL3 plasma level was 56.4 ± 8.8 pg/ml in patients with CLL cells that used unmutated IgVH (mean ± SEM, n=123) versus 14.5 ± 2.4 in patients with CLL cells that used mutated IgVH (mean ± SEM, n=139, p<0.001). The mean CCL4 level was 171.4 ± 26.3 in patients that had CLL cells that used unmutated IgVH and 92.5 ± 17.5 in patients that had CLL that expressed mutated IgVH. On the other hand, the relative absolute white cell count or presence of chromosomal abnormalities did not correlate with high plasma levels of CCL3 or CCL4. Immunohistochemistry revealed that CCL4 was predominantly expressed in proliferation centers in approximately 50% of the cases. Currently, we are evaluating whether high plasma levels of CCL3 and/or CCL4 are associated with a relatively short time from diagnosis to requiring initial treatment by the IWCLL-working group criteria. Also, we are exploring whether high plasma levels of CCL3 or CCL4 are associated with high proportions of infiltrating T cells in proliferation centers.
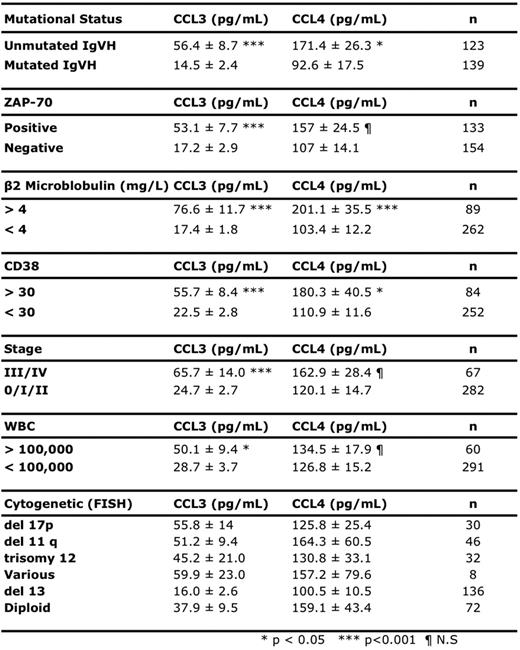
These studies suggest that patients can be stratified by their relative plasma levels of CCL3 and/or CCL4 and that high plasma-levels of theses chemokines define a characteristic that may be associated with aggressive disease.
No relevant conflicts of interest to declare.
This icon denotes an abstract that is clinically relevant.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal