

Abstract
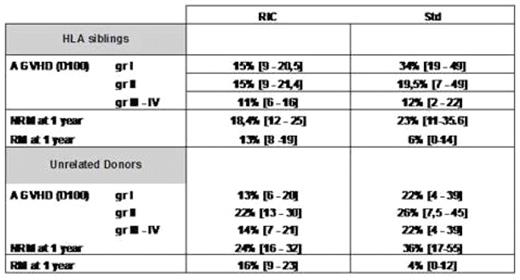
This retrospective analysis concerned 374 patients (pts) who underwent an allogeneic HSCT for CLL reported to the EBMT registry. There were 282 males (75%) and 92 females with a median age of 53 years (24–69). The interval between diagnosis and transplantation was 53 months (3–308). Forty-five pts (12%) have received a previous HSCT. At transplant, 302 among 323 evaluated patients had a good performance status (PS) (93%), 51 pts were in CR (14%), 163 in PR (45.5%), 39 in SD (11.5%) and 105 in PD (29%) among 353 evaluated patients. Two hundred and ninety-two pts received a standard (Std) and 82 a reduced intensity conditioning regimen (RIC); 314 pts received PBSC, 55 BM and 5 cord blood cells from 202 HLA siblings (Sib), 2 mismatched related donors and 170 unrelated donors (UD). There were 136 (36%) sex-mismatched (90 F/M and 46 M/F), 150 pairs (40%) had an ABO incompatibility (61 minor, 99 major) and for CMV: 80 pairs were +, 148− and 112 mixed. After transplantation, 359 pts engrafted, 201 pts developed an AGVHD (gr I: 76, gr II : 79, gr III: 30 and gr IV:16) and 153 presented a cGVHD (75 limited and 78 extensive). At day 100 after transplant, the cumulative incidence of AGVHD for the total population was 17% (13–22) for gr I, 31% (26–36) for gr ≥ II. [Sib: 19% (13–25) gr I and 27% (21–34) gr ≥ II; UD: 16% (9–22) gr I and 38% (29–47) gr ≥ II]. Results concerning the cumulative incidence of AGVHD according to HLA typing and kind of conditioning are shown in Table I. At 1 year after transplant for the total population, the cumulative incidence of limited and extensive cGVHD were 15 % (6–24) and 29.5% (18–41) for Std; 18.6 (13–24) and 18% (13–23) for RIC respectively. With a median follow up of 38 months, the probability of 3-year and 5-year overall survival (OS) and disease-free survival (DFS) for the total group were 56% (51–62) and 47.4 % (42–53); 49 % (43–56) and 42% (36–48.5) respectively. We observed a significant difference concerning 5-year OS according to the pretransplant disease status [CR: 73% (60–89), PR: 57% (48–68) and PD: 35% (26–46)] (p<0.00001). There was no significant difference between standard and RIC HSCT in term of OS with 52.4 % (42–66) and 47% (40–55.5) respectively (p=0.44) (Figure 1) [Std and RIC Sib: 51% (37–70) and 56% (47–67); Std and RIC UD: 60% (44–83) and 40% (29–55) respectively]. The multivariate analysis using Cox model showed a significant impact of 3 factors on OS: age: HR=1.061 (1.02–1.10) p<0.0001, gender: HR=2.29 (1.02–5.11) p=0.04 and PS: HR=3.15 (1.40–7.10) p=0.005. The cumulative incidence of non-relapse and relapse mortality (NRM and RM) at 3 months and 1 year after transplant were: 10 % (7–13), 5% (3–7) and 24% (19–28), 15% (12–19) respectively [Std:23 % (11–35.6), 6% (0–14) 1 year; RIC: 22.5% (17.5–27), 18% (13–22) at 1 year]. Results concerning the cumulative incidence of NRM and RM according to HLA typing and kind of conditioning are shown in Table I. This large retrospective analysis showed a high percentage of long-term OS after HSCT for CLL either after Std or RIC conditioning without any difference between the 2 groups except for the AGVHD (gr I, III and IV) where we had an higher incidence in the Std group, and for the RM with a higher level in the RIC group. Moreover, we demonstrated the important impact of disease status pretransplant (univariate); age, PS and sex-matching (multivariate) on the global OS.
Table 1: cumulative incidence of AGVHD, NRM and RM according to HLA typing and kind of conditioning
Figure

Probability of OS for Standard conditioning group and RIC group
Disclosures: No relevant conflicts of interest to declare

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal