

Abstract
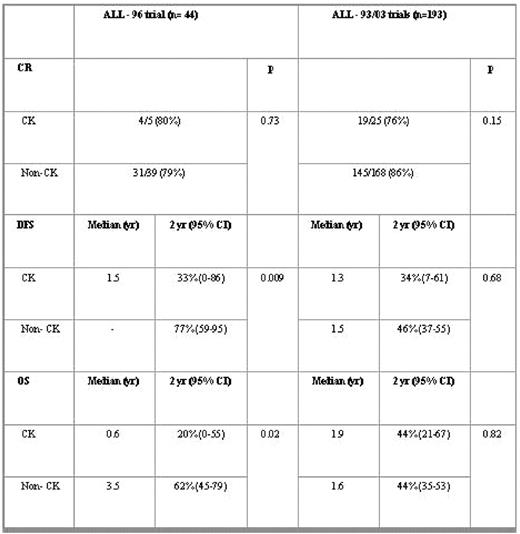
Different from acute myeloblastic leukemia, the prognostic significance of complex karyotype (CK) is not well known in adults with ALL. A recent study showed that CK (≥5 chromosomal abnormalities) confer an increased risk of treatment failure and poor survival (Moorman, 2007). The aim of study was to analyze the possible prognostic influence of CK in Ph- adult (≥15yr) ALL patients treated with risk-adapted protocols from the Spanish PETHEMA Group. The cytogenetic studies were reviewed following the ISCN criteria (2005). CK was defined as the finding of 3 or more structural chromosomal abnormalities. Patients were included in three different trials: ALL-96 for standard-risk (SR) ALL, and ALL-93 or ALL-AR03 for high-risk (HR) ALL. Patients with Burkitt’s ALL were not included in these trials. Patients included: 237. SR: n=44, 25 males, WBC count 12x109/L (SD: 14), 5 patients with CK (11.4%), 39 non-complex karyotype and normal karyotype (non- CK) (88.6%). HR: n= 193, 107 males, WBC count 58x109/L (SD: 77), 25 patients with CK (13%), 168 non- CK (87%). Complete remision (CR), disease free survival (DFS) and overall survival (OS) according to karyotype group and trial are showed in Table: When CK was defined as the finding of ≥ 5 structural chromosomal abnormalities (n=11, SR=3, HR=8), DFS and OS were also significantly shortened in patients with SR ALL and CK (p=0.007 and p=0.001, respectively), but not in patients with HR ALL. Complex karyotype (defined as ≥ 3 or ≥5 structural chromosomal abnormalities) did not have any prognostic relevance in adults with high-risk Ph- ALL, whereas a significant short survival observed in standard-risk patients with complex karyotype.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal