

Abstract
The incidence of cGVHD is likely to continuously increase as a result of the increasing use of allo-SCT (especially with reduced-intensity conditioning regimens) in older patients, peripheral blood stem cells as stem cell source, and frequent donor lymphocyte infusions, all of which are known to increase the risk of cGVHD. Standard primary treatment of cGVHD remains a combination of corticosteroids (CS) and calcineurin inhibitors. There is no standard therapy for those who fail to respond to CS, and CS-resistant GVHD is associated with high morbidity. The aim of this report was to analyze the outcome of patients treated with RTX as salvage therapy for refractory cGVHD. 15 consecutive patients experiencing severe or refractory GVHD received IV infusions of RTX (375mg/m2/infusion) at weekly intervals for 4 weeks. Responding patients were allowed to receive additional courses of maintenance therapy. Response to RTX was assessed one month after the last infusion. Patients’ characteristics, GVHD features and outcome are summarized in the Table below. RTX was administered at a median time of 178 (range, 69–1136) days after allo-SCT, and patients received a median of 5 (range, 1–12) infusions. Most have received and failed at least 2 lines of immunosuppressive therapy prior to RTX. With a median follow-up of 118 days (range, 21–834) from first infusion of RTX, no major toxicities directly related to RTX were observed. Overall, 10 patients responded to RTX administration (66%; 95%CI, 42–90%) with 3 complete remissions. In those responding patients, the patient felt improvement as soon as one week after the first RTX infusion. In addition, RTX allowed a significant reduction of CS dosage (range, 0–83%). 4 patients did not respond and died from refractory GVHD, while one responding patient died of disease progression. With a median follow-up of 461 days from onset of cGVHD (range, 91–1192), the actuarial survival rate from the first RTX infusion was 60% at one year. We conclude that despite its limited size, this cohort demonstrates evidence of beneficial activity of RTX, mainly in the classical cutaneous, mucosal and liver cGVHD. Patients with involvement of other sites are not likely to benefit much from RTX. Results achieved with RTX in the cGVHD refractory setting, pave the way for further developments. As such, the addition of RTX to prednisone for the initial treatment of cGVHD is worth further investigations, both to increase the overall response rate, and to enable a more rapid CS taper while incurring less long-term toxicity.
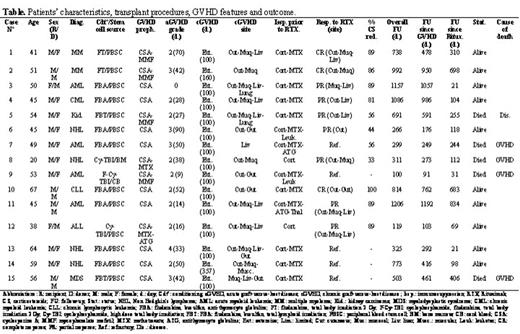
Patients’ characteristics, transplant procedures, GVHD features and outcome.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal