

Abstract
In the setting of AML, RIC regimens have emerged as an attractive modality to decrease toxicity. However, toxicity might represent only one aspect of the problem, since AML encompasses a group of chemosensitive diseases, raising concerns that significant reduction of the intensity of the preparative regimen, while increasing immunosuppression, may have a negative impact on long-term outcome. This report describes the comparative results of 31 AML patients in CR1 receiving RIC allo-SCT from an HLA-identical sibling in 2 institutions (Nantes, n=13; and Marseille, n=18) using 2 different “global” treatment approaches (Table below). After achievement of CR1, the “Nantes” approach included administration of one or two courses of consolidation with high-dose cytarabine (HDC), followed immediately by allo-SCT conditioned with a genuine nonmyeloablative, but highly immunosuppressive RIC regimen including fludarabine, low dose busulfan (4 mg/Kg), ATG (5 mg/Kg) and both CsA and corticosteroids for GVHD prophylaxis (“FB1A2” group). The “Marseille” program aimed to deliver after CR1, in addition to HDC, an autologous SCT followed by allo-SCT conditioned with fludarabine, an intermediate dose of busulfan (8 mg/Kg), low dose ATG (2.5 mg/Kg) and CsA alone for GVHD prophylaxis (“FB2A1” group). In the “FB2A1” group, 12 patients (67%) could actually receive the planned auto-SCT. With a median follow-up of 47 months, leukemia-free survival (LFS) in the whole study population was 56% at 5 years. However, the KM estimate of LFS was significantly higher in the “FB2A1” group as compared to the “FB1A2” group (P=0.01; 72% vs. 31% at 5 years). Overall, 8 patients (26%; 95%CI, 11–41%) had relapsed at a median of 320 (range, 241–707) days after diagnosis, and the significant difference between the 2 groups in terms of LFS was likely due to a higher risk of leukemia relapse in the “FB1A2” group (6/13, vs. 2/18; P=0.07). Five patients died from toxicity, for an overall incidence of TRM of 16% (95%CI, 6–34%), with this being comparable between the 2 groups (2/13 vs. 3/18; P=NS). Such comparable TRM despite a more “intensive” approach, translated towards a higher overall survival in the “FB2A1” group as compared to the “FB1A2” group (72% vs. 42% at 5 years; P=0.07). After controlling for relevant factors, in the multivariate analysis, actual performance of auto-SCT prior to RIC allo-SCT (P=0.04; RR=4.9; 95%CI, 1.1–22.4), was significantly predictive of an improved LFS. We conclude that RIC allo-SCT from an HLA-matched related donor represents a valid option for AML patients not eligible for standard allo-SCT. However, in order to achieve optimal results, a comprehensive treatment “package” including some form of high dose therapy prior to RIC allo-SCT and/or semi-intensive cytoreduction/myeloablation incorporated within the RIC regimen is likely necessary to allow sufficient time for the GVL effect.
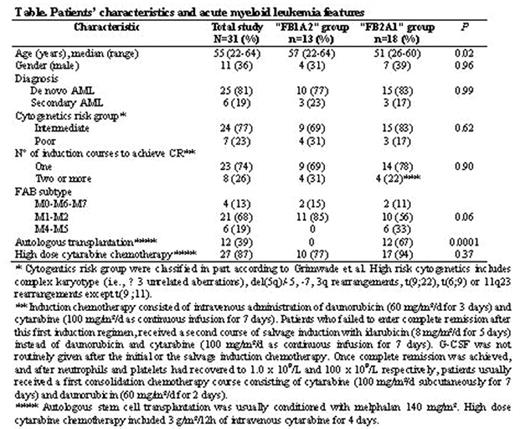
Patients’ characteristics and acute myeloid leukemia features

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal