

Abstract
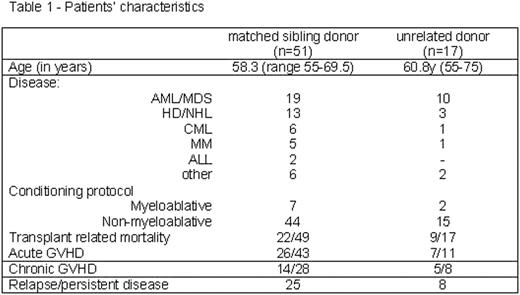
Most of the hematological malignancies where allogeneic stem cell transplantation (SCT) is a therapeutic option occur in elderly patients. Additionally, in this age group, the probability of finding a matched sibling donor decreases due to mortality and co-morbidities of patient’s siblings which may exclude them from donation. In such case, SCT from an unrelated donor (UD) can offer a therapeutic solution for elderly patients in need although such a procedure is considered more hazardous than SCT from a matched sibling (mostly due to procedure and GVHD related morbidity and mortality). We present our data on transplantation, in 68 elderly (age>/= 55 years) patients that underwent SCT from a matched sibling (n=51) or UD (n=17) mostly using fludarabine-based regimen (table 1).
Median recipient age was 58.3y in the sibling group and 60.8y in the UD group (NS) (range 55–69.5y and 55–75y, respectively). With a median follow-up of 40 months of the survivors after sibling SCT, the 1-year OS was 32%. Similarly, in the UD group the 1-year OS was 35% (survivors’ median follow-up 48.5m) (NS). Transplant related mortality occurred in 22/49 (45%) and 9/17 (53%) of the patients transplanted from sibling or UD respectively (NS). Occurrence of acute GVHD was noted in 26/43 and 7/11 (figure 1) evaluable patients transplanted from matched sibling or UD respectively (NS). Diagnosis of chronic GVHD was made in 50% (14/28) and 63% (5/8) of the patients in the sibling and UD group correspondingly. GVHD related mortality occurred in 11 and 2 patients, respectively.
We conclude that using fludarabine based regimen, allogeneic SCT from an UD is equally effective as in patients undergoing SCT from matched family member. Age per-se should not be currently used as an exclusion criterion for either initiation of donor search or SCT from UD.

Disclosure: No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal