

Abstract
Background: The majority of cases of peripheral neuropathy related to monoclonal gamopathy of unknown significance (MGUS) are of the IgM type. Neuropathy associated with antibodies to myelin-associated-glycoprotein (anti-MAG) accounts for 50% of IgM-related neuropathies. Anti-MAG related neuropathies often improve after treatment with human Ig (IVIG), or a combination of cyclophosphamide (cytoxan) and plasma exchange. But this improvement is often short-lived, expensive, and the repeated doses of cytoxan may predispose patients to an increased risk of infections and secondary malignancies. Therefore, efficacious and less toxic treatment approaches are needed in anti-MAG-related neuropathies. We postulated that Rituximab treatment would eradicate the autoantibody producing B-cell lymphocyte clone in patients with IgM antibody-related neuropathies and thereby reduce the titers of neurotoxic antibodies.
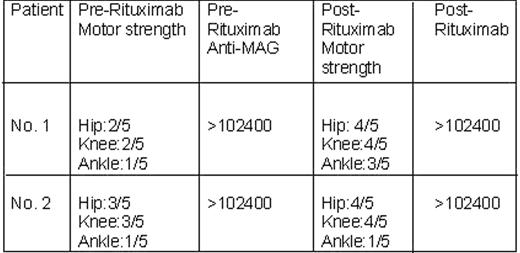
Methods: Two patients followed at the Kansas City Veterans Affair Medical Center neuromuscular clinic with diagnoses of MGUS and IgM antibody-related neuropathies were evaluated by history, physical examination, electrodiagnostic evaluation, and serum testing. Both patients had sensory-motor (mixed) neuropathies characterized by slowly progressive asymmetric weakness, muscle wasting, areflexia, and sensory loss. These patients also had elevated anti-MAG titers and were previously treated with plasma exchange, Cytoxan, IVIG, resulting in a good clinical improvement of their symptoms. The clinical remissions, however, were short lived (3–6 moths). Both the patients were then treated with four weekly IV infusions of Rituximab (375 mg/M2).
Results: During the ensuing 12 months after Rituximab treatment, both patients had subjective and objective sensory and motor neurological improvement, however, the degree of improvement was variable. We noticed no change in the titers of anti-MAG levels despite clinical improvement. Based on our experience we postulate that the clinical improvement may not correlate with changes in the anti-MAG titers. Moreover, it could be possible that the recovery of anti-MAG titers may lag behind the clinical improvement. Results for both the patients are formulated below in the table. The graph depicts the anti-MAG titers and physical strength of one of the treated patient in relationship to the Rituximab treatment.
Conclusion: Rituximab is a relatively safe and efficacious therapy for patients with IgM antibody-directed polyneuropathies. Additional large scale, prospective studies with a longer follow-up are needed to develop Rituximab as a targeted therapy against anti-MAG neuropathies.

Disclosure: No relevant conflicts of interest to declare.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal