

Abstract
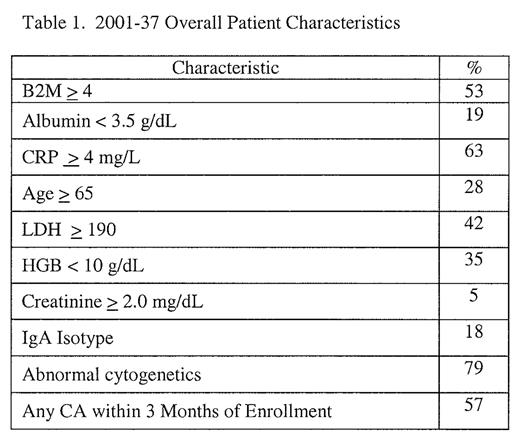
Based on an index patient who responded to V 1.0 mg/m2 + T 100 mg upon progression on V alone and documented prior resistance to T, a phase 1–2 trial was initiated of the V+T combination in patients with advanced and refractory MM, 79% with a history of cytogenetic abnormalities (CA) including 57% pre-V, 81% with one and 52% with 2 prior transplants (n=79). Due to concerns for synergistic neurotoxicity, V was initially given at a dose of 1.0 mg/m2 on days 1, 4, 8 and 11; with the second cycle on day 21, T was introduced at incremental doses, per cohorts of at least 10 patients, at 50, 100, 150 and 200 mg daily. In the absence of grade 3 neurotoxicity, V was then increased to 1.3 mg/m2 and the same T dose escalation scheme was applied. Accrual to the 7th cohort with V 1.3 mg/m2 + T 150 mg has been completed. Distribution of cohorts is as depicted in the attached table per V and T dose along with overall characteristics. First cycle PR to V alone was 25% including 10% achieving n-CR; maximum response was noted after completion of 2 additional cycles with combined V + T: 40% achieved PR and ~ 20% n-CR, 60% had ≥ 25% M protein reduction. Analysis of response rates by V and T cohorts (V 1.0 mg/m2, n=45; V 1.3 mg/m2, n=34) and T dose (T ≤ 100 mg, n=42; > 100 mg, n=37) revealed no significant differences in response rates: median EFS for all 79 patients is 7 mos and median OS 21 (at 12 mo 67% alive). On multivariate analysis of 17 potentially relevant prognostic markers, prior therapy > 5 yrs (36% of patients) was associated with improved survival (HR 0.4, p=.03) whereas prior T (78% of patients) was associated with inferior post-V+T survival (HR 4.1, p=.05). In addition, V 1.3 mg/m2 reduced the risk of events (HR 0.6, p=.07) and of death (HR 0.3, p=.02).


This feature is available to Subscribers Only
Sign In or Create an Account Close Modal