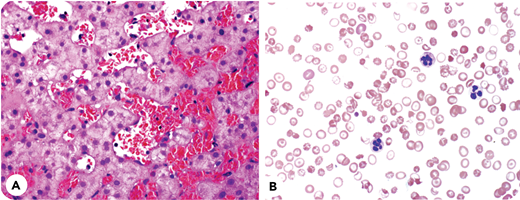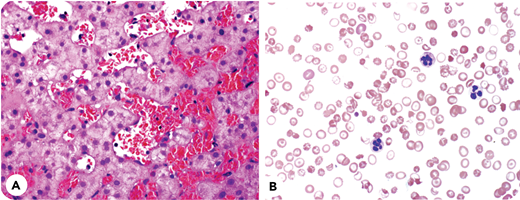
A 24-year-old man with sickle cell anemia and only 1 prior hospitalization presented in 2010 with increasing jaundice. Examination revealed intense jaundice and hepatomegaly. Hemoglobin was 7.2 g/dL; reticulocytes, 11%; ALT, 32 U/L; alkaline phosphatase, 573 U/L; and bilirubin 32, mg/dL overwhelmingly conjugated. Despite red blood cell (RBC) exchange transfusion (RBEX), bilirubin remained >30 mg/dL. Liver biopsy (panel A; hematoxylin and eosin stain, ×40 objective) showed marked sinusoidal dilatation with distention by numerous sickled RBCs. There was minimal canalicular cholestasis, focal mild ballooning degeneration of hepatocytes, scant reticuloendothelial iron, and focal mild perisinusoidal fibrosis, without hepatocyte necrosis or trabecular atrophy. In clinical context, the findings were interpreted as sickle cell intrahepatic cholestasis. Notwithstanding regular outpatient RBEX and supportive measures for 10 years, liver disease progressed to cirrhosis, ascites, and encephalopathy. Even with posttransfusion hemoglobin A >90% and functional asplenia, spur cells emerged (panel B; Wright Giemsa stain, ×60 objective). The patient is now recovering from a liver transplant.
This case vividly illustrates the rare complication of sickle cell cholestatic hepatic failure and the unique emergence of spur cell anemia despite an asplenic state. When acute hepatic sickle crises do not respond to RBEX, the outlook may be ominous. Pathophysiology remains obscure. Spur cell morphology results from cholesterol and phospholipid aberrations in RBC membranes, predicting imminent mortality unless liver disease can be reversed.
A 24-year-old man with sickle cell anemia and only 1 prior hospitalization presented in 2010 with increasing jaundice. Examination revealed intense jaundice and hepatomegaly. Hemoglobin was 7.2 g/dL; reticulocytes, 11%; ALT, 32 U/L; alkaline phosphatase, 573 U/L; and bilirubin 32, mg/dL overwhelmingly conjugated. Despite red blood cell (RBC) exchange transfusion (RBEX), bilirubin remained >30 mg/dL. Liver biopsy (panel A; hematoxylin and eosin stain, ×40 objective) showed marked sinusoidal dilatation with distention by numerous sickled RBCs. There was minimal canalicular cholestasis, focal mild ballooning degeneration of hepatocytes, scant reticuloendothelial iron, and focal mild perisinusoidal fibrosis, without hepatocyte necrosis or trabecular atrophy. In clinical context, the findings were interpreted as sickle cell intrahepatic cholestasis. Notwithstanding regular outpatient RBEX and supportive measures for 10 years, liver disease progressed to cirrhosis, ascites, and encephalopathy. Even with posttransfusion hemoglobin A >90% and functional asplenia, spur cells emerged (panel B; Wright Giemsa stain, ×60 objective). The patient is now recovering from a liver transplant.
This case vividly illustrates the rare complication of sickle cell cholestatic hepatic failure and the unique emergence of spur cell anemia despite an asplenic state. When acute hepatic sickle crises do not respond to RBEX, the outlook may be ominous. Pathophysiology remains obscure. Spur cell morphology results from cholesterol and phospholipid aberrations in RBC membranes, predicting imminent mortality unless liver disease can be reversed.
For additional images, visit the ASH Image Bank, a reference and teaching tool that is continually updated with new atlas and case study images. For more information, visit http://imagebank.hematology.org