

Introduction:
The outbreak of a novel infection, COVID-19, has greatly impacted the well-being of individuals worldwide. Persons with sickle cell disease (SCD) constitute a vulnerable population, subject to health disparities, who may have worse outcomes from COVID-19. Within the United States, New York has a large population of patients with SCD. Here, we analyze the clinical course and outcomes of SCD patients with COVID-19 who were admitted to a community teaching hospital in Brooklyn, NY.
Methods:
We conducted a retrospective chart review of adult patients with SCD hospitalized with laboratory- confirmed COVID-19. Electronic health records were reviewed to identify patients and analyze their clinical course. Clinical characteristics, laboratory and radiology data were assessed. Rates of acute chest syndrome (ACS), acute kidney injury (AKI) and venous thromboembolism (VTE) were determined. ACS was defined by the presence of fever and/or respiratory symptoms accompanied by a new pulmonary infiltrate on chest Xray. Data on use of blood transfusion, treatments, length of stay and mortality were collected.
Results:
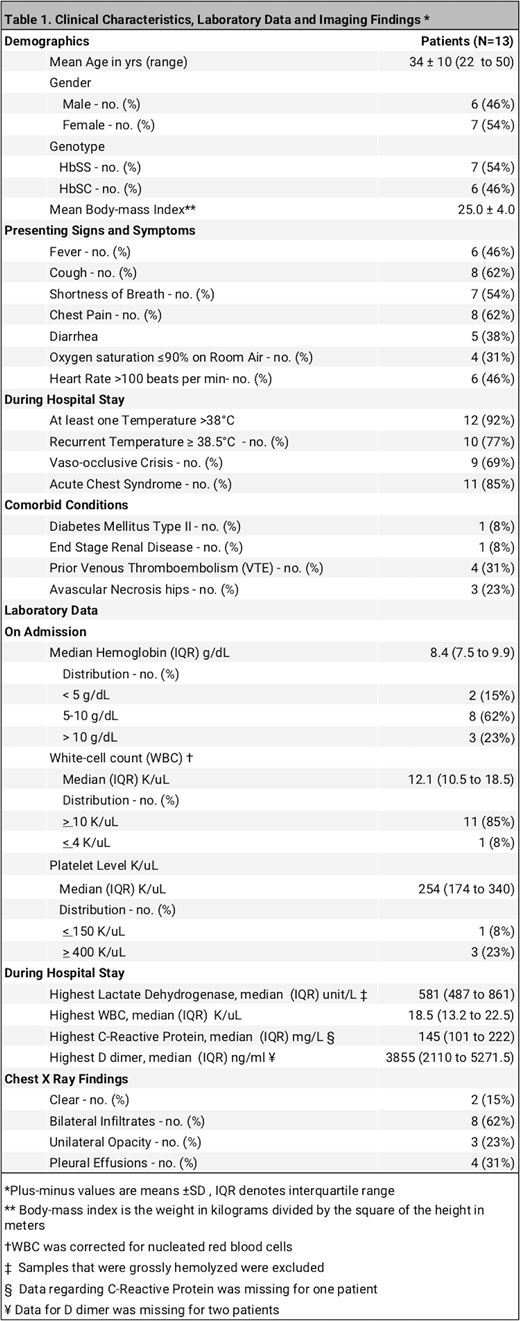
Between March 1 to June 30, 2020, 53 adults with SCD were hospitalized at our institution. Of these, 13 patients had COVID-19 infection. The mean (±SD) age of the COVID-19 patients was 34±10 years (range, 22 to 50) with 54% being female. Seven patients (54%) were Hb SS, and 6 patients (46%) were Hb SC. Comorbid conditions included Diabetes Mellitus (1 patient), SLE (1), End-stage renal disease (1), prior VTE (4) and Avascular necrosis of hip (3). Four patients were on hydroxyurea.
Clinical, laboratory and radiological findings are summarized in Table 1. While all the Hb SS patients presented with vaso-occlusive crisis, 4 of the 6 patients with Hb SC did not have symptoms of pain crisis. Chest pain and cough were the most common symptoms at presentation. During the hospital stay, 12 patients (92%) had at least one febrile episode >38°C, with 77% having recurrent fevers above 38.5°C.
Eleven patients (85%) met criteria for ACS. Seventy-seven percent of all patients required supplemental oxygen. Nine patients (69%) were transfused, with 4 patients undergoing exchange transfusion. Sixty-seven percent of the transfused patients were transfused within 48 hours of admission. No patients required intubation or mechanical ventilation and none were admitted to the intensive care unit (ICU). Five patients (38.5%) received hydroxychloroquine while 84.6% were treated with antibiotics. No patient received remdesivir.
Three patients (23%) developed AKI: of these, one patient required acute hemodialysis, the other two cases were mild with peak creatinine less than 2.0 mg/dl.
Ninety-two percent of patients received prophylactic anticoagulation with either unfractionated heparin, enoxaparin or fondaparinux. One patient who did not receive an anticoagulant due to thrombocytopenia developed an acute deep vein thrombosis which was also catheter-related. Of note, during the initial phase of the pandemic standard dosing of prophylactic anticoagulants were used but in the later months, some patients received higher prophylactic doses in keeping with hospital protocol.
The median length of hospital stay was 9.4 days (interquartile range, 8.1 to 13.3). There were no deaths - all patients were discharged home.
Summary:
Panepinto et al (Emerg Infect Dis.) reported a mortality of 7% in 178 SCD patients with COVID-19 in the United States. Other published reports have detailed more favorable outcomes (Arlet et al, Lancet and Appiah-Kubi et al, Br J Haematol.). In this small retrospective analysis of hospitalized SCD patients, there was no mortality. Acute chest syndrome was the most common complication observed. VTE and severe AKI were infrequent. Blood transfusion was performed in the majority of patients (69%); two thirds of the patients transfused received blood within 48 hours of hospitalization. There were no ICU admissions and no use of mechanical ventilation indicative perhaps of less severe COVID-19 disease. This may have been due to the young age of the cohort. Early use of blood transfusion may have been a factor in reducing disease severity and improving outcomes. The best approach to managing these patients is unclear. We advocate for the development and dissemination of evidence-based guidelines to manage SCD patients with COVID-19 to reduce morbidity and mortality in this at-risk population.
No relevant conflicts of interest to declare.

