


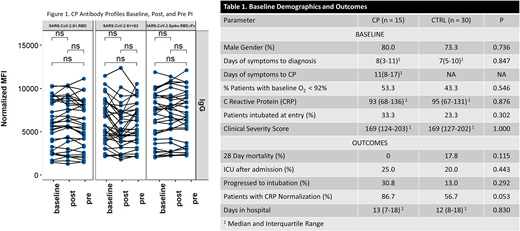
Background. COVID-19, caused by the SARS-CoV-2 virus, is a pandemic disease with high morbidity and mortality. Currently, available therapeutic options for COVID-19 are limited. Prior experience in epidemics with convalescent plasma (CP) containing antibodies to viruses has demonstrated variable indications of therapeutic efficacy for: Influenza, Argentine Hemorrhagic Fever, and SARS. Characterizing antibody titers to viruses has indicated correlation with therapeutic efficacy. Convalescent COVID-19 patients with potent SARS-CoV-2 antibody responses can serve as plasma donors for immune therapy. However, antibody responses are variable, many donors are first-time higher risk blood donors, and rapid assays to select optimal CP immune efficacy are limited. Pathogen inactivation (PI) of CP can reduce the risk of transfusion-transmitted infection by unrecognized pathogens. Objectives. This study characterized COVID-19 PI-CP activity; and evaluated efficacy and safety of PI CP transfusion in a case matched controlled cohort of acute COVID-19 patients. Methods. COVID-19 apheresis CP (650 - 1300 mL) was collected from nasopharyngeal PCR + outpatients following 2 PCR negative tests or 28 days after symptom resolution. Amotosalen-UVA PI of CP (INTERCEPT Blood System for Plasma) was performed, and antibody efficacy before and after PI was characterized by: VSV reporter pseudo-virus plaque neutralization (RVPN) NT-50 titer (Vitalant Research Institute, San Francisco), antibody to S and N virus proteins by agglutination-dependent antibody PCR (ADAP, Enable Biosciences, San Francisco), virus ACE-2 soluble receptor neutralization assay (Enable Biosciences), and SARS-CoV-2 antibody profile by coronavirus microarray (University of California, Irvine). Patient inclusion criteria were: confirmed SARS-CoV-2 infection, hospitalization, pulmonary infiltrates, availability of ABO compatible CP, and informed consent. CP patients were matched with control patients (CTRL) for disease severity at diagnosis by standardized clinical risk score (W. Liang et al JAMA Intern Med 2020) and concomitant Tocilizumab use. CP Patients received a total of 400 mL of PI CP from 2 donors over 48 hours and standard therapy. CTRL patients received standard COVID-19 therapy without CP. The primary outcome was in-hospital death to day 28. Secondary outcomes included: progression to intubation, admission to ICU, time to discharge, serious adverse events, NP viral clearance, plasma viral clearance, and humoral immune responses. Differences between CP and CTRL patients were assessed by the Mann-Whitney test for continuous variables, and by Fisher's exact test for categorical variables. Progression to ICU and intubation were analyzed as odds ratios calculated by conditional logistic regression. Results. 15 CP and 30 CTRL patients were enrolled. One CP patient was admitted in cardiogenic shock. Only 2 of 15 CP cohort patients had detectable IgG antibody to SARS CoV-2 S1 antigen at study entry. 3 of 15 PI CP donors had negligible SARS CoV-2 IgG antibodies to all antigens, and demonstrated poor neutralization efficacy. 12/15 CP had effective RVPN titers (> 1:80), RVPN titers were correlated with ACE-2 neutralization antibody titers (r2 = 0.83), and had significant activity specific for S and RBD antigens by microarray profiling (Figure 1). SARS CoV-2 antibody levels were variable between CP donors, but not impacted by PI (Figure 1). Baseline characteristics of CP and matched CTRL patients were similar (Table 1). Sensitivity analysis was performed assessing mortality after exclusion of one CTRL patient admitted in cardiogenic shock and the 2 respective controls. In-hospital 28-day mortality was lower in the CP cohort (0/14) compared to 5/28 CTRL, p = 0.151, 2-sided Fisher's exact test. Progression to intubation, ICU admission, and days in hospital were not significantly different (Table 1). There was a trend toward decreased inflammatory response (CRP normalization) in CP patients. Conclusions. In hospital mortality of COVID-19 patients was lower in the PI-CP cohort, but not statistically significant. 15% of CP had ineffective antibody by multiple assays. However, PI did not impact CP anti-SARS-CoV-2 activity. PI of plasma provides reduced risk of transfusion transmitted infection from COVID-19 CP donors. In this study, PI CP was safe, and may be effective for early treatment of hospitalized COVID-19 patients.
von Goetz:Cerus Corporation: Current Employment, Current equity holder in publicly-traded company. Khan:Nanommune Inc.: Current equity holder in private company. Tsai:Enable Biosciences: Current Employment. Robinson:Enable Biosciences: Current Employment. Seftel:Enable Biosciences: Current Employment, Current equity holder in private company. Bagri:Cerus Corporation: Current Employment, Current equity holder in publicly-traded company. Corash:Cerus Corporation: Current Employment, Current equity holder in publicly-traded company.
This icon denotes a clinically relevant abstract

