

Introduction:
The identification of driver mutations has dramatically changed the management of myeloid malignancies. More recently, mutations have been identified in RNA splicing machinery in myelodysplastic syndrome (MDS) and acute myeloid leukemia (AML) (Yoshida et al. 2011). Recurring missense mutations have been observed in the RNA splicing factor 3B subunit 1 (SF3B1), serine and arginine-rich splicing factor (SRSF2) and U2 small nuclear RNA auxiliary factor 1 (U2AF1). In this study, we sought to decipher the disease-specific features and clinical outcomes of individual spliceosome mutations in patients with MDS and AML.
Methods:
We conducted a retrospective observational study of 40 patients with one or more mutations in 3 spliceosome genes (SRSF2, U2AF1, SF3B1) from the University of Massachusetts (UMass) Leukemia Registry. Demographics, peripheral blood data, clinical parameters such as treatment offered including bone marrow transplant and response to chemotherapy was longitudinally recorded. We performed clonal dynamic modeling to identify clonal evolution in individual patients with spliceosome-mutant MDS or AML.
Results:
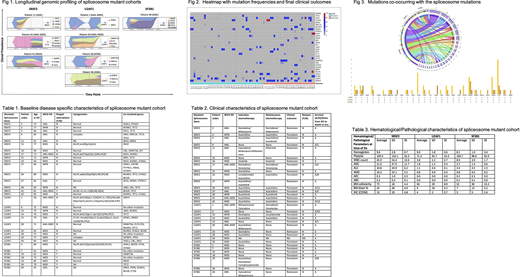
Longitudinal data was available for 83% (33/40) patients with an average follow up duration of 91 weeks. Average age at diagnosis was 75±4 years which was consistent across the 3 mutational cohorts. A mortality of ~35% was observed in our cohort (Table 2). MDS was diagnosed in 48% (19/40), AML and AML-MRC were diagnosed in 33% (13/40) and 13% (5/40), respectively (Table 1). SRSF2 was the most common spliceosome mutation (50%) and SF3B1 and U2AF1 were equally divided in the remainder. Cytogenetic abnormalities were found in 5/33 (15%) in SRSF2, 4/33 (12%) in U2AF1, and 1/33 (3%) in the SF3B1 groups. Of the 16 patients with SRSF2-mutant hematological conditions, 7/16 (40%) had persistent disease (PD) which was similar across the other two spliceosome genes. Compared to U2AF1- and SF3B1-mutant patients, SRSF2-mutant patients presented with a higher WBC count (mean 45.9 x 103/mcl ± 13.6 x 103/mcl), higher bone marrow (BM) cellularity (73% ± 4.4%), and higher BM blast percentage (24% ± 6.9%) at the time of diagnosis (Table 3), which was independent of the FLT3 status. The most commonly recurring co-occurring mutants with SRSF2 were TET2 (occurred 8/16 times along with SRSF2 with a rate of 50%), IDH2 (31%), STAG2 (25%) and RUNX1 (25%). In the U2AF1-mutant cohort, RUNX1 (30%) and TET2 (20%) were the most frequent co-mutants. In the SF3B1 cohort, BCOR (29%) and KRAS (29%) were the most frequently mutated and shared few co-occurring mutations with SFSR2-mutant and U2AF1-mutant cohorts as demonstrated in the circosplots (Figure 3). The heatmap further elaborates this association and alludes to a possible genetic signature associated with favorable or adverse clinical outcomes (Figure 2).
Conclusion:
This study deciphers among SRSF2-, U2AF1-, and SF3B1-mutant MDS/AML and demonstrates that SRSF2-mutant MDS/AML presents with higher WBC count, BM cellularity, and BM blast burden. SRSF2-mutant MDS/AML carries the most dismal prognosis amongst the spliceosome mutations. The co-mutational landscape of SF3B1-mutant MDS/AML is distinctly different from SRSF2 and U2AF1 cohort. While we only identified 1 individual with SF3B1 mutation with longitudinal data and hence no meaningful conclusion is possible, SRSF2 cohort shows poor response to standard chemotherapy in 2/3 individuals (Figure 1). We also found that BRAF and CEBPA are not co-occurring mutations within the spliceosome-mutant cohort, suggesting mutual exclusivity (Figure 2). While our understanding of MDS/AML expands, new drugs are constantly under development and have led to significant improvements in the disease outcome in younger patients. Seiler et al recently studied a new oral drug H3B-8800, which binds the SF3B complex in a competitive manner and has demonstrated potent inhibition and lethality of the spliceosome-mutant cells (Seiler et al. 2018). After demonstration of survival advantage in vivo in murine models, the drug is now in Phase 1 clinical trial which is pending completion soon. Our dataset provides clinical correlates of spliceosome-mutant AML/MDS in a longitudinal fashion and also alludes to a possible genetic signature associated with favorable or adverse outcomes in these patients.
No relevant conflicts of interest to declare.

