

Introduction: Nearly 20% of all newly identified cases of VTE is associated with cancer. Hematologic malignancies are at increased risk of developing VTE. We aimed to identify the prevalence of hematologic malignancy in VTE patients and compare the survival between VTE and non-VTE patients with or without hematologic malignancy.
Methods: Using linked administrative data and a validated algorithm we identified adult VTE cases in Alberta, Canada from 2003 to 2015. We also identified patients without VTE using the same database. Subjects having ICD-10 code for hematologic malignancy and solid tumor within one year before and after the VTE index event were further identified. Cox proportional hazard regression model was applied to estimate the hazard ratio (HR) of death. The Kaplan Meier survival analysis was performed to compare survival rate among patients with different diagnosis.
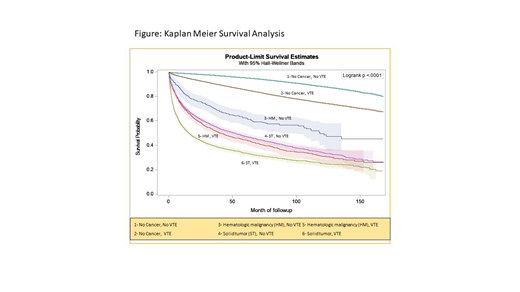
Results: We identified 56,907 VTE patients. Of them 37,876 (66.6%), 18,502 (32.5%) and 529 (0.9%) cases were diagnosed as deep vein thrombosis (DVT), pulmonary embolism (PE), and both DVT & PE respectively. 57.4% of the VTE patients were female. Of all VTE cases, 1647 (2.9%) patients had hematologic malignancies and 5034 (8.8%) patients had solid tumor. Of the hematologic malignancy cases 853 (51.8%) , 164 (10%), 105 (6.4%), 302(28.3%) and 223 (13.5%) had Lymphoma, leukemia, myelodysplastic syndrome (MDS), myeloproliferative neoplasm (MPN) and plasma cell dyscrasia respectively. We identified 27,664 patients without any diagnosis of VTE. Among them 586 (2.1%) and 4065 (14.7%) patients had hematologic malignancy and solid tumor, respectively. In VTE group, the hazard of death for patients with hematologic malignancy and solid tumor were 5.2 (95% CI: 4.8-5.5) and 7.5 (95% CI: 7.2-7.8) times greater than that of patients with no cancer, respectively. In the patients with no VTE, hazard of death among people with hematologic malignancy and solid tumor were 7.4 (95% CI: 6.4-8.5) and 12.4 (95% CI: 11.6-13.2) times greater than that of people with no cancer, respectively. In all hematologic malignancy and solid tumor patients, the hazard of death for patients with VTE were 1.8 (95% CI: 1.5-2.1) and 1.6 (95% CI: 1.5-1.7) times greater than that of patients with no VTE, respectively. In all patients without any cancer, those with VTE had 2.6 (95% CI: 2.4-2.7) times increased hazard of death than those without VTE. The Kaplan Meier survival analysis showed the lowest survival probability among VTE patients with solid tumor and hematologic malignancy (Log rank p<0.0001).
Conclusion: Lymphoma is the most common hematologic malignancy in VTE patients. VTE patients with any type of malignancy have an increased hazard of death compared to those without VTE.
Wu:BMS-Pfizer: Honoraria; Bayer: Other: Local PI for trial ; Leo Pharma: Honoraria; BMS-Pfizer: Other: Local PI for trial ; Daiichi-Sankyo: Other: Local PI for trial ; Pfizer: Honoraria; Servier: Honoraria.

