Background
Multiple myeloma (MM) is a frequent hematologic malignancy. The current gold standard frontline strategy includes a proteasome inhibitor (PI)-based induction, followed by autologous stem cell transplant (ASCT).
Access to novel drugs in Latin America (LA) is limited. ASCT is available in most countries, but real access to it is highly heterogeneous. Data regarding patients´ outcomes in candidates to ASCT in the region is scarce.
The aim of this study was to describe clinical characteristics and outcomes of MM transplant eligible patients in LA countries.
Material and Methods
Retrospective international multicenter cohort study. Consecutive MM transplant- eligible patients diagnosed between 2010 and 2018 from participating centers in Chile, Argentina, Ecuador, Mexico, Colombia, and Uruguay were included. Data were collected from clinical records in a standardized report form. We analyzed clinical characteristics at diagnosis and frontline therapy outcomes, including ASCT.
Transplant-eligible patients were defined as fit patients younger than 66 years old.
Active MM and response to treatment were defined according to current IMWG criteria.
Inclusion criteria:
1.- Patients with newly diagnosed active MM between 2010 and 2018.
2.- Older than 18 years, and younger than 66 years.
3- Candidates for ASCT according to the evaluation of the attending physician
Exclusion criteria:
1- Lack of minimum data in the clinical history
2- Plasma cell leukemia, AL amyloidosis or solitary plasmacytoma.
3- HIV infection
4-No consent and/or Ethics Committee approvals.
Statistical analysis
A descriptive statistic has been done. Comparisons of characteristics between groups was made usingT-student, Chi2 or ANOVA, as appropriate. Survival analysis was performed using Kaplan-Meier curves. Comparisons of survival between groups were made by the logarithmic recording method and the calculations of the risk relationships by Cox regression.
Statistical analysis was performed by using STATA 13.
Results
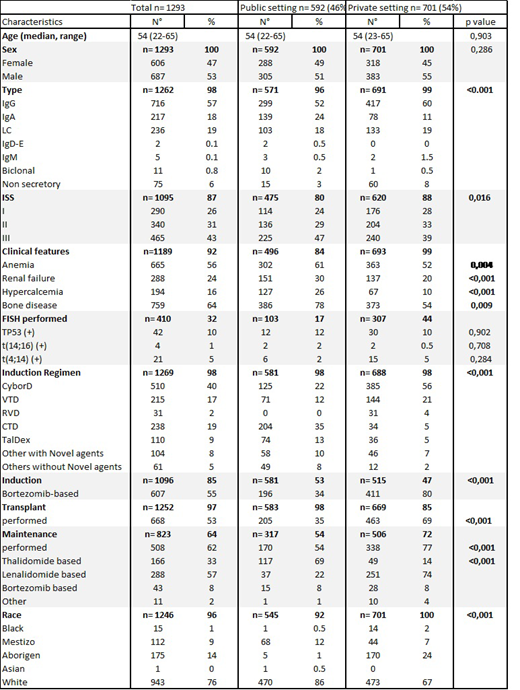
We included 1293 patients in the study, 363 from Chile, 395 from Argentina, 209 from Colombia, 45 from Ecuador, 151 from Mexico, and 130 from Uruguay. The main characteristics at diagnosis and therapeutic strategies are shown in Table 1. Optimal response (sCR, CR and VGPR) was achieved in 38% of the patients in the cyclophosphamide, bortezomib, and dexamethasone (CyBorD) group, in 46% in the bortezomib, thalidomide, and dexamethasone (VTD) group, and in 36% in the cyclophosphamide, thalidomide, and dexamethasone (CTD) group, the 3 main induction regimens used. Only 53% of patients finally received ASCT.
Significant differences were found between both groups, private and public institutions, regarding burden of symptoms, ISS staging, access to PI based induction, ASCT completion and adequate maintenance, with patients from the latter being more symptomatic, and receiving suboptimal therapy.
FISH analysis was performed in less than 50% of patients, both in the public and private setting.
With a median follow up of 34 months (range 1-113), median overall survival (OS) was 86 months. The 5-year progression free survival (PFS) was 38% and 5- year overall survival (OS) was 64%. When comparing public vs private settings, 5 year OS was 45% vs 80%, with a median OS of 56 months vs not reached, respectively (P<0,0001).
In the multivariable analysis renal failure (p=0.03), achieving less than VGPR response (p<0.0001), not undergoing ASCT (p=0.001), and not receiving maintenance (p=0.005) were independent factors associated with worse outcome.
Conclusion
This is the largest report on transplant eligible patients with MM in LA. Great inequities are shown between public and private health systems.
Survival in transplant-eligible patients is lower than that described in other regions.
Only one third of patients had FISH performed. This means that very few patients are treated with a risk-based induction in LA.
Patients in the public setting are diagnosed with a more symptomatic disease, probably due to a late diagnosis. OS is significantly worse in the public setting. This might be explained by the significant differences in access to PI-based induction, ASCT and maintenance between private and public institutions, with patients from the latter receiving suboptimal frontline therapy and maintenance.
Reasons for 47% of potential candidates not being transplanted merit further analysis.
Peña:Novartis: Other: Congress inscription and flights; Tecnofarma: Other: Congress inscription and flights; Roche: Other: Congress inscription and flights; Biotoscana: Other: Congress inscription and flights; Janssen: Other: Congress inscription and flights; Pfizer: Membership on an entity's Board of Directors or advisory committees. Rojas:Roche: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees; Pfeizer: Membership on an entity's Board of Directors or advisory committees; Abbvie: Membership on an entity's Board of Directors or advisory committees. Abello:Takeda: Other: Participation in advisory board meeting. Gomez-Almaguer:Amgen: Consultancy, Speakers Bureau; Janssen: Consultancy, Speakers Bureau; Teva: Consultancy, Speakers Bureau; Takeda: Consultancy, Speakers Bureau; Celgene: Consultancy, Speakers Bureau.