


Introduction: The advent of Tyrosine Kinase Inhibitors (TKI) changed the treatment paradigm of Philadelphia chromosome Positive (Ph+) Acute Lymphoblastic Leukemia (ALL). Different treatment strategies exist including combinations of TKI with steroids or with intensive multi-agent chemotherapy regimens. We present here our institutional experience of a "ramp-up" strategy using dasatinib with steroids as induction followed by the combination of dasatinib plus the intensive chemotherapy schema of HyperCVAD alternating with HD MTX/cytarabine.
Methods: We performed a retrospective review of the electronic medical records of adult patients (pts) treated in our institution for Ph+ ALL. We collected and analyzed data for pts with Ph+ ALL treated with dasatinib and steroids followed by dasatinib plus HyperCVAD alternating with HD-MTX/cytarabine.
Results: We identified 25 pts that were treated with the ramp-up treatment approach between 2014-2019. The median age at diagnosis was 45 years old (range 21-65 years old). Fifty-two percent were women and 60% white. Diagnosis of Ph+ ALL was based on FISH analysis with karyotype being positive for the Ph+ chromosomal abnormality in 64% pts; 8% of pts had cryptic translocation and rest not available ( N/A). Sixty percent of pts had p190 Bcr/Abl transcript, 16% had p210 and 8% N/A (including 2 pts that Bcr/Abl transcript was undetectable despite morphological disease). The CD20 by multicolor flow cytometry (MFC) was positive in 16%, heterogenous in 20%, and low/negative in the rest (64%). Eighty-four percent of pts had a WBC less than 50K/cmm at diagnosis; median WBC was 17K/cmm (range 0.8 -131.4 K/cmm). All pts except one received induction with initial dose of 140 mg of dasatinib daily; 84% received prednisone and rest received dexamethasone followed by prednisone. For those pts on dasatinib 140 mg daily, only 2 required adjustment/brief interruption during induction.
Eighty-four percent of pts achieved morphological CR, 8% CRp, and 8% had residual ALL post induction with dasatinib and steroids. Of the 23 pts achieving CR/CRp, 34% had minimal residual disease (MRD) by MFC, 26% by FISH analysis and 86% by PCR for Bcr/Abl transcript (21 evaluable pts). Median time from initiation of induction to response bone marrow assessment was 26 days (range 14 - 40 days;75% percentile 28 days).
All 25 pts proceeded with HyperCVAD alternating with HD MTX/cytarabine, and the dose of dasatinib used was 70 mg daily (aside from 1 patient who received 100 mg daily). Median time from induction to initiation of HyperCVAD was 34 days (range 17-68 days). The median number of courses (HyperCVAD or HD MTX/cytarabine) for the 25 pts was 3. The 13 pts that ultimately went to transplant in CR1 had also a median of 3 courses.
Sixty percent of pts ultimately underwent allo-HSCT. Median time to allo-HSCT from initiation of HyperCVAD was 106 days (range 66-294; 75% percentile 163 days).
Overall, all pts achieved CR/CRp with 68% of pts (from the 22 evaluable for molecular remission) attaining also undetectable Bcr/Abl PCR (complete molecular response) as a best response. All pts with post-induction residual disease achieved CR with the dasatinib/intensive chemotherapy combination.
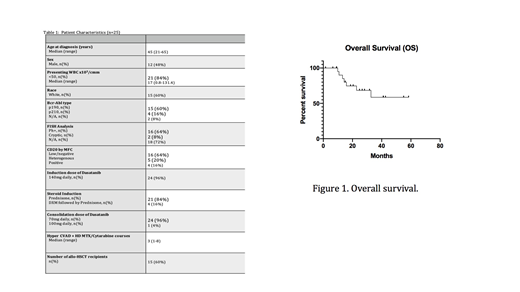
Twenty percent of pts had morphological relapse; two pts were treated for non-morphological relapse. Median time to morphological relapse was 148 days from induction (range 106-796 days). The median follow-up was 20.4 months (range 1.5 -58.4; 75% percentile 36.8 months). At last follow up 72% of pts were alive; median OS (not censored for allo-HSCT) was not reached (figure 1). There were no deaths in the first 60 days.
Conclusion: Induction therapy with dasatinib and steroids was overall well tolerated and was associated with a very favorable CR/CRp rate, with only a minority of pts requiring treatment adjustment. Subsequent consolidation with dasatinib and HyperCVAD alternating with HD-MTX/cytarabine (+/- allo-HSCT) led to deep remissions in 68% of the pts. Sixty percent of pts underwent allo-HSCT and the median OS was not reached and with no deaths in the first 60 days.
Hence, induction therapy with dasatinib and steroids followed by dasatinib plus HyperCVAD alternating with HD-MTX/cytarabine can be considered for Philadelphia chromosome-positive ALL pts to achieve deep remissions with low early mortality.
Vachhani:AbbVie: Membership on an entity's Board of Directors or advisory committees; Agios: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Astellas: Speakers Bureau; Daiichi Sankyo: Membership on an entity's Board of Directors or advisory committees; Incyte: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau. Costa:Fujimoto Pharmaceutical Corporation Japan: Other: Advisor; Amgen: Consultancy, Honoraria, Research Funding, Speakers Bureau; Janssen: Research Funding, Speakers Bureau; Celgene: Consultancy, Honoraria, Research Funding; Sanofi: Consultancy, Honoraria, Speakers Bureau; GSK: Consultancy, Honoraria, Research Funding; Abbvie: Consultancy; Karyopharm: Consultancy. Erba:Amgen, Celgene, Daiichi Sankyo, ImmunoGen, Incyte, Jazz Pharmaceuticals, Millennium, Novartis, Ono, Pfizer, Seattle Genetics, Sunesis: Consultancy; Celgene, Incyte, Novartis: Speakers Bureau; Agios, Amgen, Astellas Pharma, Daiichi Sankyo, ImmunoGen, Janssen, Jazz Pharmaceuticals, Juno, Millennium, Seattle Genetics: Research Funding. Papadantonakis:Agios: Consultancy, Honoraria.
This icon denotes a clinically relevant abstract

